
"Independently Completed Region's First Case: 9-Hour Radical Resection of High-Complexity Hilar Ch
"Independently Completed the First Case in the Prefecture - 9-Hour Marathon" - Highly Complex Hepatic Hilar Cholangiocarcinoma Radical Surgery
General Surgery - Hepatobiliary Chapter: Radical Resection of Hilar Cholangiocarcinoma (Bismuth-Corlette Type IIIB) Independently Completed in Prefecture-Level City, Gansu
Patient: Shang xx (male), 70 years old.
Presenting Complaint: Admitted for "yellowing of skin and sclera for 15 days, accompanied by skin itching for 1 week". Pre-admission Investigations (Wuwe External Hospital):
● Abdominal CT: Suggestion of malignancy in left hepatic duct and common hepatic duct (Cholangiocarcinoma/Ca), causing mild intrahepatic biliary dilatation; gallbladder not visualized.
● Abdominal MRI:
◦ Truncation of the common hepatic duct with an adjacent nodule showing abnormal signal; cholangiocarcinoma highly suspected.
◦ Gallbladder not visualized.
● Liver Function Tests:
◦ Total Bilirubin: 157.20 umol/L
◦ Indirect Bilirubin: 44.90 umol/L
◦ Direct Bilirubin: 112.30 umol/L
◦ Aspartate Aminotransferase (AST): 168 U/L
● Past Medical History:
◦ Hypertension for 8 years, highest BP 180/110 mmHg. Long-term medication: Nifedipine Sustained-Release Tablets and Metoprolol Tartrate Sustained-Release Tablets.
◦ Diabetes Mellitus for 1 year, highest blood glucose 22.0 mmol/L. Long-term regular oral Metformin, with suboptimal glycemic control.
◦ Appendectomy 26 years ago.
◦ Left great saphenous vein surgery for varices 28 years ago.
◦ Traumatic cataract surgery 5 years ago.
◦ Gout for 8 years.
◦ Coronary heart disease status post coronary artery stent implantation 5 years ago.
◦ Epididymitis surgery 4 months ago.
Admission Investigations:
● Liver Function Tests:
◦ Total Bilirubin: 283.3 umol/L
◦ Direct Bilirubin: 206.10 umol/L
◦ Alanine Aminotransferase (ALT): 112 U/L
◦ Aspartate Aminotransferase (AST): 68 U/L
Pre-operative Management:
Pre-operative Biliary Drainage:Ultrasound-guided Percutaneous Transhepatic Intrahepatic Biliary Drainage (PTCD) was performed due to significantly elevated bilirubin.
Comorbidity Management: Endocrinology and Cardiology consultations obtained; active management initiated for hypertension and blood glucose control.
Surgical Decision Process:
After thorough review of imaging studies, the Department Director concluded the tumor was resectable but acknowledged significant surgical risk.The patient's family expressed a strong desire for surgical intervention.Following extensive discussion within the department and subsequent hospital-wide Multidisciplinary Team (MDT) consultation, a consensus recommendation for surgical treatment was reached. After detailed communication outlining the risks and benefits with the patient's family, informed consent for surgery was obtained.

Hilar Cholangiocarcinoma (HCCA), also known as Klatskin tumor, is a common malignant tumor of the biliary system. Due to its specific location at the hepatic hilum, infiltrative growth pattern, and close relationship with the portal vessels, surgical resection of HCCA poses significant difficulties and challenges. Some experts vividly compare pancreaticoduodenectomy (the Whipple procedure) to the "crown" of general surgery. In this analogy, radical resection of hilar cholangiocarcinoma can be considered the most brilliant jewel on that crown—especially for Type IIIA, the even more challenging Type IIIB, and the most difficult Type IV hilar cholangiocarcinoma.

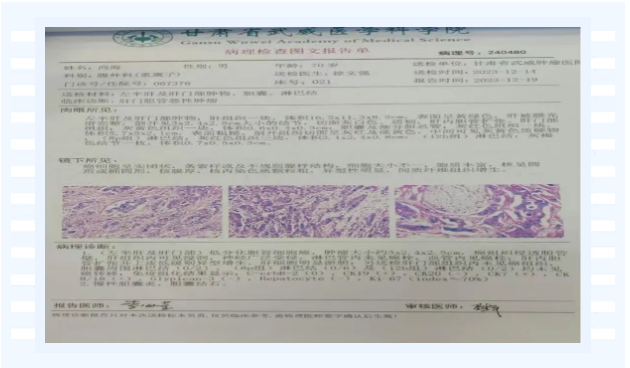
Postoperative Pathology Report:
1.(Left Hepatic Lobe & Porta Hepatis): Poorly Differentiated Cholangiocarcinoma.Tumor dimensions: approximately 3.0 x 2.4 x 2.5 cm.The carcinoma has invaded through the bile duct wall.Hepatic tissue invasion is identified.Extensive perineural invasion is present.No tumor emboli are identified within lymphatic vessels.Tumor emboli are present within blood vessels (vascular invasion).Intrahepatic bile ducts are dilated and exhibit low-grade epithelial dysplasia.Marked hepatocellular cholestasis is present.Additionally submitted porta hepatis tissue shows no evidence of carcinoma.Lymph Nodes Status:Pericholecystic lymph nodes (0/2): Negative for metastasis.Group 8p lymph nodes (0/6): Negative for metastasis.Group 12b lymph nodes (0/2): Negative for metastasis.Immunohistochemistry (IHC) Results:C-erbB-2 (HER2/neu): 0 (Negative)CK19: +CK20: -CK7: +CK8/18: +Glypican-3: -Hepatocyte: -Ki-67: Proliferative index ≈70%
2.Chronic Cholecystitis with Gallstones.
Surgical Procedure:
- Duration: 9 hours.
- Estimated Blood Loss (EBL): 300 mL.
- Postoperative Recovery: The patient recovered well and was discharged.
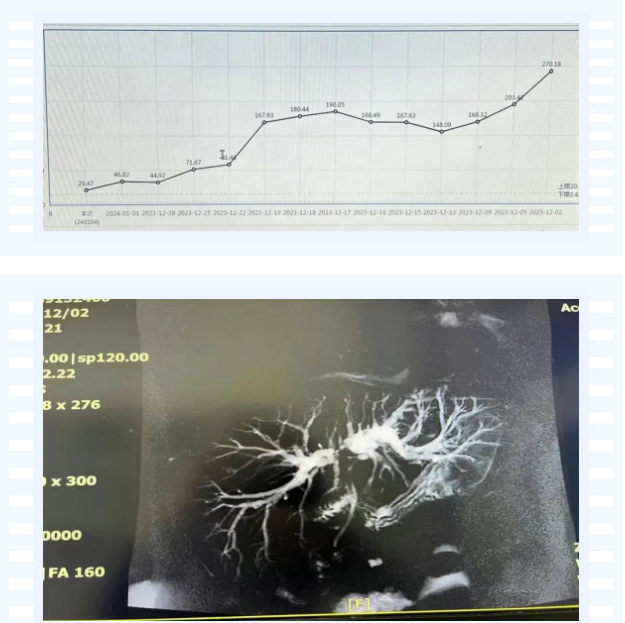
Preoperative and Postoperative Changes in Total Bilirubin
Hilar cholangiocarcinoma (HCCA), also known as Klatskin tumor, is a common malignant tumor of the biliary system. Due to its unique location at the hepatic hilum, infiltrative growth pattern, and close proximity to critical hilar vascular structures, surgical resection of HCCA presents significant challenges and difficulties. Experts vividly describe the pancreaticoduodenectomy (Whipple procedure) as the "crown jewel" of general surgery, while radical resection for hilar cholangiocarcinoma can be considered the most brilliant gem in that crown—particularly for complex cases such as Type IIIA, Type IIIB, and even the more technically demanding Type IV HCCA.

Li Shigong, Academic Leader
Associate Chief Physician. Former Director of Hepatobiliary Surgery at Wuwei Cancer Hospital; currently Director of Abdominal Surgery and Director of General Surgery at Wuwei Cancer Hospital. Trained at Shanghai Eastern Hepatobiliary Surgery Hospital and Shanghai Ruijin Hospital, he previously served as Director of General Surgery and Director of Hepatopancreatobiliary & Splenic Surgery at Wuwei Medical College Cancer Hospital, and later as Director of Abdominal Surgery at a major tertiary hospital in Chongqing.
Specializing in traditional open surgeries, laparoscopic procedures, and robotic-assisted interventions for gastrointestinal, hepatobiliary, and pancreatic tumors, he has performed over 4,000 abdominal operations to date. Among the first in the province to perform laparoscopy-assisted pancreaticoduodenectomy, he routinely conducts:
● Laparoscopic radical gastrectomy
● Laparoscopic radical resection of colorectal cancer
● Hepatic tumor and hemangioma resections
● Complex open and minimally invasive surgeries for biliary/pancreatic tumors, including pancreaticoduodenectomy.
Department of Abdominal Surgery
Team Structure:
● Associate Chief Physicians: 2
● Attending Physicians: 1
● Resident Physicians: 3
Clinical Expertise:
1. Diagnosis and treatment of hepatopancreatobiliary malignancies and benign conditions (e.g., intra/extrahepatic bile duct stones, gallstones)
2. Management of gastric and colorectal cancers
3. Emergency care for acute abdominal conditions (intestinal obstruction, incarcerated hernias, appendicitis, gastrointestinal perforation, pancreatitis, abdominal trauma)
4. Treatment of hepatopancreatobiliary and splenic disorders (portal hypertension, hypersplenism, splenomegaly)
Surgical Scope:
● Open & Minimally Invasive Surgeries:
▶ Radical gastrectomy and colorectal resection
▶ Hepatic tumor resection; combined pancreatic-splenic tumor resection
▶ Multi-organ resection for gastric/colorectal cancer with liver metastasis
▶ Radical cholecystectomy; pancreaticoduodenectomy for pancreatic/duodenal/biliary tumors
▶ Radical resection for hilar cholangiocarcinoma
● Laparoscopic Procedures:
▶ Cholecystectomy for gallstones; hernia repair; other general surgery operations

Contact Information
Department Phone: +86-935-6989803
▶ Li Shigong: +86-150-2592-7869
▶ Tao Jichun: +86-138-3053-9708
▶ Sun Yanfeng: +86-138-8455-4011
