
After undergoing an ECG and cardiac ultrasound, why do I still need a coronary angiography?
After undergoing an ECG and cardiac ultrasound, why do I still need a coronary angiography?
When you experience heart discomfort and have completed an ECG and cardiac ultrasound, only for your doctor to recommend a "coronary angiography," it’s natural to feel puzzled: weren’t the first two tests fine? Why is this additional step necessary? Don’t worry—it’s like troubleshooting a problem at home. Different tools have different specialties, and each is indispensable. Today, let’s explore how these three tests differ and why they’re all important.
The "Three Musketeers" of Cardiac Exams: Each with Its Own Strengths
1. Electrocardiogram (ECG/EKG)
—— The Heart’s "Electrical Circuit Inspector"

- Function: Captures the heart’s electrical signals, similar to checking if the wiring at home is functioning properly.
- Detects best: Irregular heartbeats (arrhythmias), myocardial ischemia (during angina or heart attack), and signs of past heart attacks.
- Limitations: The test duration is short and can only capture issues at the moment of testing. If ischemia is "episodic" (e.g., occurring only during intense activity), a standard ECG may appear entirely normal. It’s like an electrical fault that only happens during peak usage—if the electrician arrives when everything seems fine, the problem won’t be detected.
2. Cardiac Ultrasound (Echocardiography)
—— The Heart’s "Structural Engineer"

- Function: Uses ultrasound to visualize the heart’s structure and motion in real time, like inspecting whether a building’s framework is stable or if its doors and windows (valves) open and close properly.
- Detects best: Heart size, myocardial thickness, pumping function (ejection fraction), valve function, pericardial effusion, and congenital heart defects.
- Limitations: It cannot directly visualize the coronary arteries! While it can show myocardial movement, if a region of the heart muscle is weakened or nonfunctional due to chronic ischemia or necrosis, it may indirectly suggest a problem with the corresponding coronary artery. However, this is only an "indirect inference"—it cannot determine which vessel is blocked, how severe the blockage is, or its exact location. It’s like seeing cracks in a wall and suspecting a foundation issue, but further inspection is needed to identify which pillar is affected and the extent of the damage.
3. Coronary Angiography (CAG)
—— The Blood Vessels’ "Pipeline Endoscope"
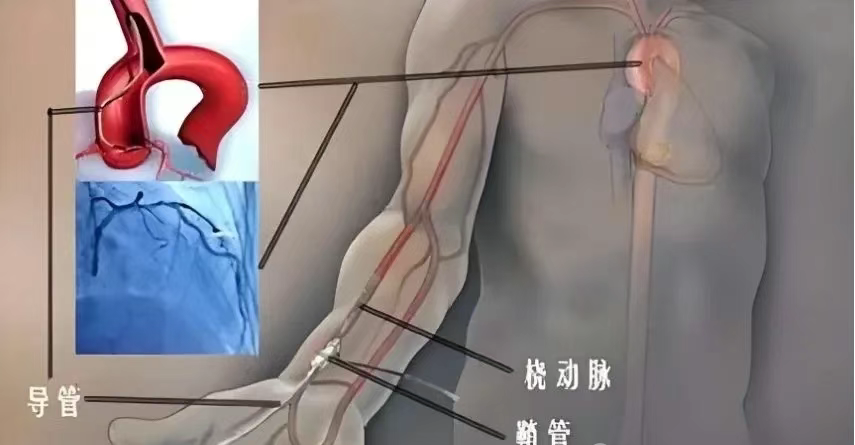
- Function: Currently the gold standard for diagnosing coronary artery disease. A thin, flexible tube (catheter) is inserted through a blood vessel in the wrist or groin and guided to the coronary arteries. Contrast dye is injected, and X-ray imaging dynamically reveals the internal condition of the coronary arteries.
- Detects best: Whether the coronary arteries are narrowed, the exact location, severity (precisely quantified as a percentage), length, and extent of the narrowing, as well as the vessels’ pathways and morphology. It’s like performing an endoscopic inspection of a home’s water pipes—where plaque (scale) has built up, where blockages are, and how severe they are, all become clear.
- Features: A minimally invasive procedure (requiring local anesthesia), technically mature, and relatively safe, though it carries slightly higher risks (e.g., bleeding, contrast allergy, or vascular injury—all with low occurrence rates) compared to the first two tests.
Why Is Angiography Needed If the First Two Tests Are Normal?
This is the crux of the issue! The reasons often include:
- Your symptoms strongly suggest coronary artery disease: Classic angina (e.g., crushing chest pain during activity that resolves with rest), unexplained severe chest tightness, or shortness of breath. Even if the ECG and ultrasound show no abnormalities at the time, doctors may still suspect a coronary artery issue. A normal ECG does not rule out coronary artery disease! If coronary artery stenosis is less than 70%, a standard ECG may appear entirely normal.
- The ECG/ultrasound reveals "clues" but cannot confirm a diagnosis: ECG shows minor ST-T segment changes (suggesting possible ischemia but nonspecific).Cardiac ultrasound detects regional wall motion abnormalities (indicating potential blood supply issues to that area).These findings hint at possible coronary artery disease but lack definitive evidence, requiring angiography for a conclusive diagnosis.
- To guide precise treatment decisions: If angiography reveals severe coronary artery narrowing (typically >70–75%), especially in the left main artery or proximal segments of major vessels, doctors may recommend stent placement (PCI) or bypass surgery (CABG) to restore blood flow.If the narrowing is less severe, intensive medication and lifestyle changes may suffice. Without the clear "pipeline map" provided by angiography, doctors cannot formulate the most accurate and effective treatment plan. It’s like not knowing the location or severity of a pipe blockage—you can’t decide whether to clean, replace a section, or overhaul the entire system.
Please understand and trust your doctor’s professional judgment. When a coronary angiography is recommended, it’s to gain a precise understanding of your heart’s blood vessels and provide the most appropriate treatment. Rather than worrying, communicate openly with your doctor to understand the necessity of the test and its risk-benefit ratio, making an informed decision together for your heart health.
Health Tip: Don’t ignore heart warning signs (e.g., chest tightness or pain during activity, unexplained shortness of breath). Seeking timely medical attention is key. Modern medicine’s precision in diagnosis and treatment relies on these complementary "heart scouts."

Director Yang Wangsheng
Key Minimally Invasive Procedures in Cardiology & Interventional Medicine:
(1) Heart & Major Vessels:
Catheter-based closure for congenital heart defects (ASD/VSD/PDA); coronary artery disease intervention (PCI); pacemaker implantation for bradyarrhythmias; radiofrequency ablation for tachyarrhythmias.
Endovascular stent grafting for aortic dissection/aneurysm; endovascular repair for abdominal aortic aneurysm; stent placement for aortic ulcers/intramural hematoma.
(2) Peripheral Vascular Minimally Invasive Procedures:
Balloon angioplasty and stenting for lower extremity arteriosclerosis obliterans; renal artery stenosis angioplasty and stenting; subclavian artery stenting; thrombolysis and thrombectomy for deep vein thrombosis; inferior vena cava filter placement/removal; radiofrequency ablation and foam sclerotherapy for varicose veins; acute arterial embolism thrombectomy/thrombolysis; acute pulmonary embolism thrombectomy/catheter-directed thrombolysis; embolization for visceral artery aneurysms.
(3) Tumor Minimally Invasive & Other Procedures:
Interventional embolization for massive hemoptysis, gastrointestinal bleeding, or gynecological hemorrhage; interventional therapy for benign/malignant solid tumors (liver cancer, hepatic hemangioma, uterine fibroids, cervical cancer, soft tissue tumors, etc.); arterial infusion chemotherapy for advanced tumors; interventional diagnosis/treatment for arterial/venous angiomas; port placement/removal for cancer patients.
Address: 1st Floor, Building 1, Heavy Ion Campus, Gansu Wuwei Cancer Hospital

