
Celiac Plexus Neurolysis: Precision Relief for Upper Abdominal Cancer Pain
Celiac Plexus Neurolysis: A Minimally Invasive Technique for Precision Relief of Upper Abdominal Cancer Pain
CT‑guided celiac plexus block/neurolysis (CPB/CPN) is a commonly used minimally invasive technique for treating refractory upper abdominal pain and cancer pain. It can effectively relieve pain and reduce opioid use, with approximately 70% of patients experiencing pain improvement after the procedure. Based on clinical consensus and practice, this article provides a concise summary of the key technical points of this technique.
I. Functions of the Celiac Plexus
The splanchnic nerves, including the greater, lesser, and least splanchnic nerves, are the main afferent pathways for pain sensation from the upper abdominal viscera. The celiac plexus is the largest autonomic nerve plexus in the human body, integrating sympathetic, parasympathetic, and visceral sensory nerves. It is responsible for transmitting visceral pain signals from the distal esophagus to the transverse colon, serving as the central hub for the conduction of upper abdominal pain.
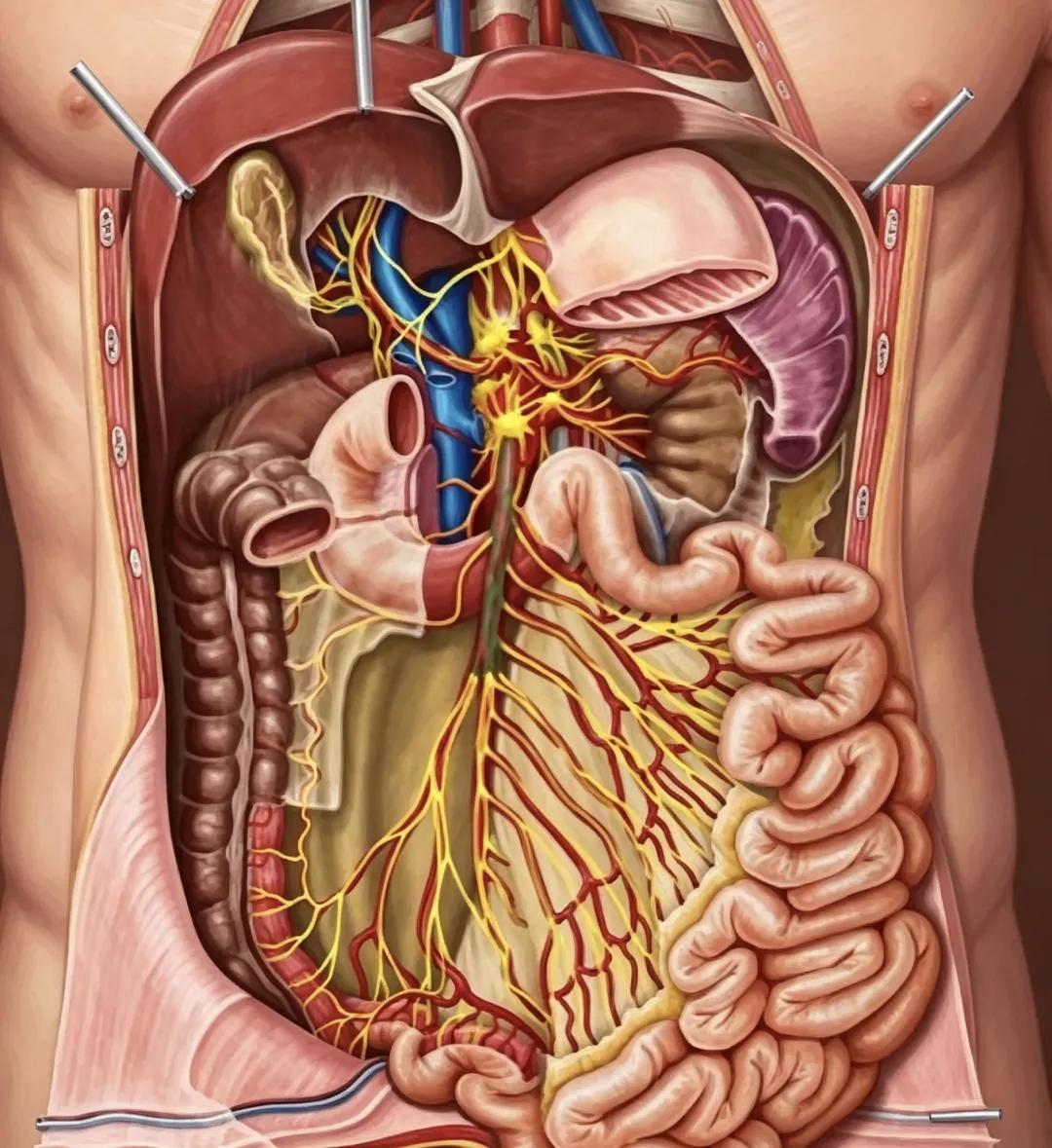
「Images generated by AI, for medical science popularization reference only」
II. Location of the Celiac Plexus
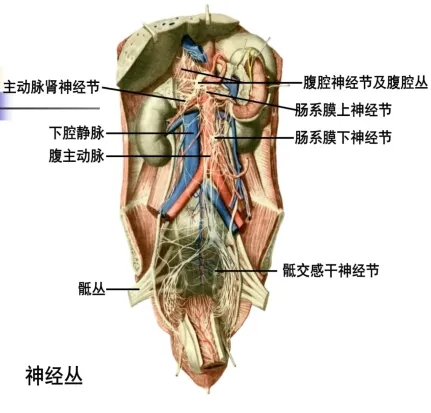
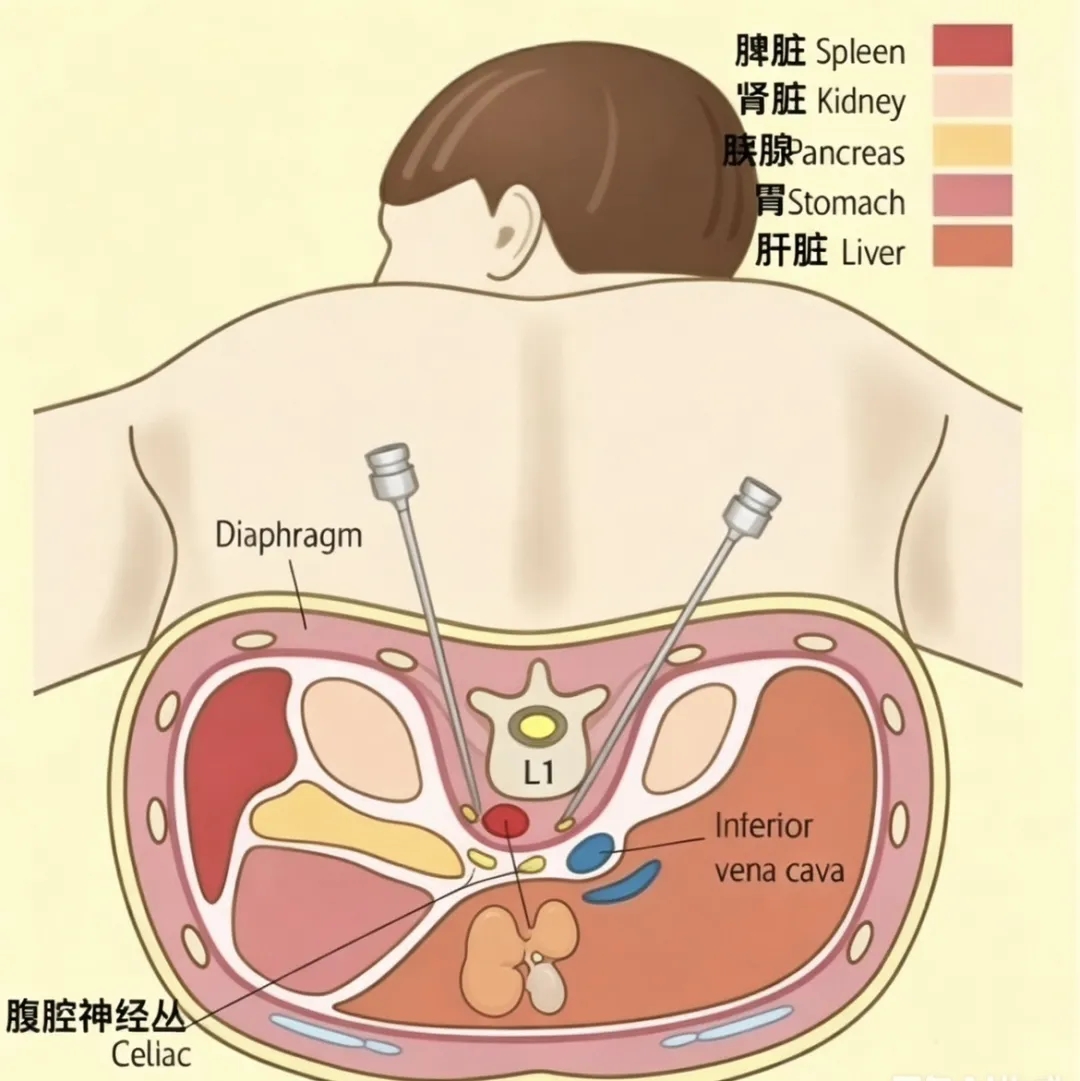
The celiac plexus is located in the retroperitoneum, anterior to the abdominal aorta, between the celiac trunk and the superior mesenteric artery, within the pre‑crural space at the level of the T12‑L1 vertebrae. It is embedded in the adipose tissue anterior to the abdominal aorta, and the celiac artery serves as the key anatomical landmark for localization.
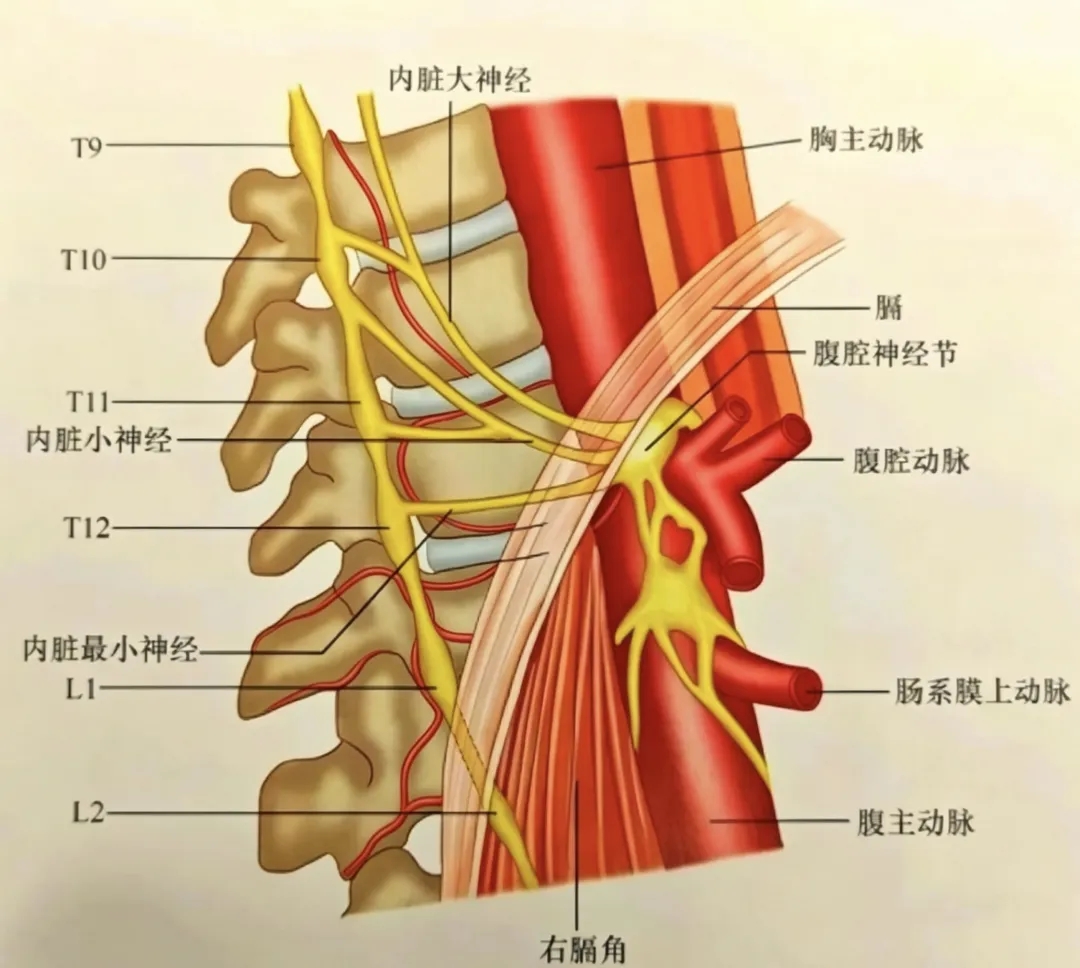
「Images generated by AI, for medical science popularization reference only」
III. Indications and Contraindications
Indications
- Cancer pain caused by upper abdominal malignancies: Refractory abdominal pain due to pancreatic cancer, liver cancer, cholangiocarcinoma, and retroperitoneal tumor metastases.
- Benign refractory abdominal pain: Chronic pancreatitis, median arcuate ligament syndrome, etc. (Neurolysis should be used with caution for benign pain.)
Contraindications
Coagulation disorders, systemic or local site infection, tumor metastasis along the puncture path, organic intestinal obstruction, severe debilitation or shock in the patient, local anatomical destruction due to tumor infiltration, and abdominal vascular anatomical abnormalities, among others.
IV. Puncture Path
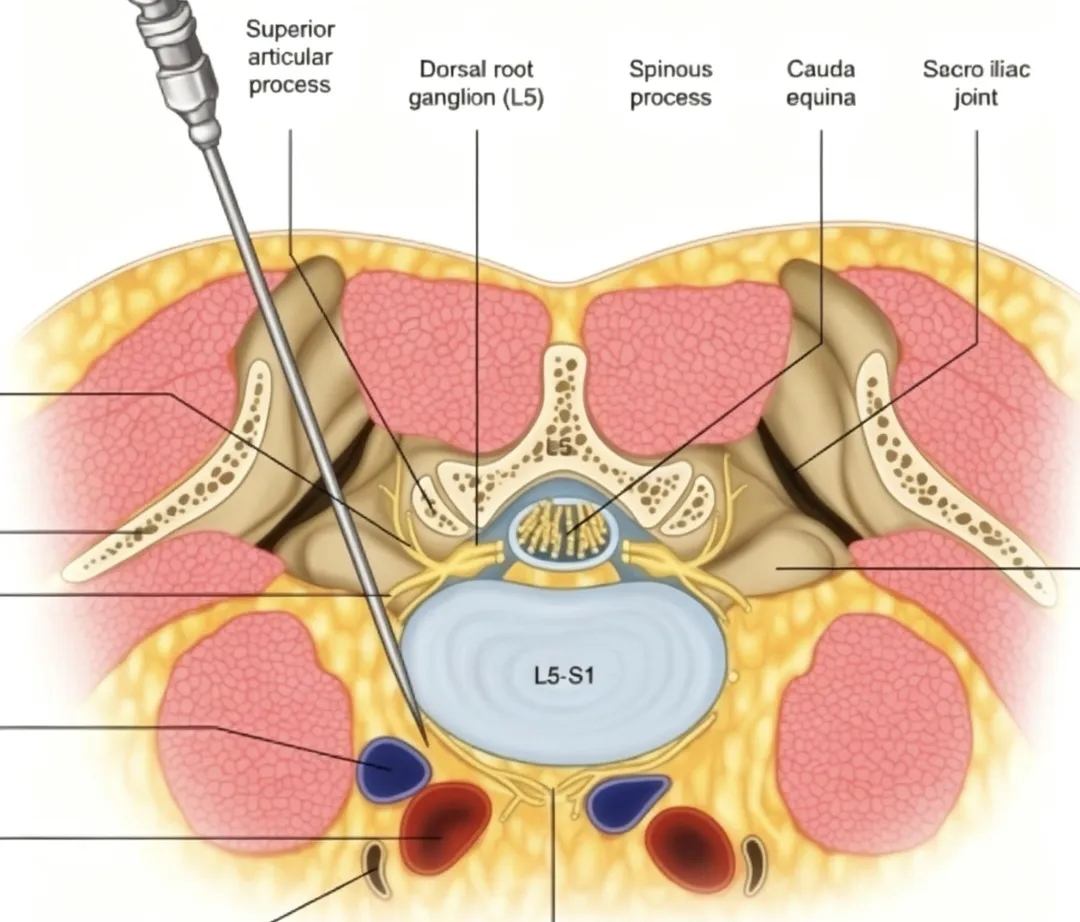
Clinically, the standard approach is CT‑guided posterior access, with the needle inserted through the patient's back. A trans‑intervertebral disc route may be used to precisely deliver the needle tip to the target site in the pre‑crural space.
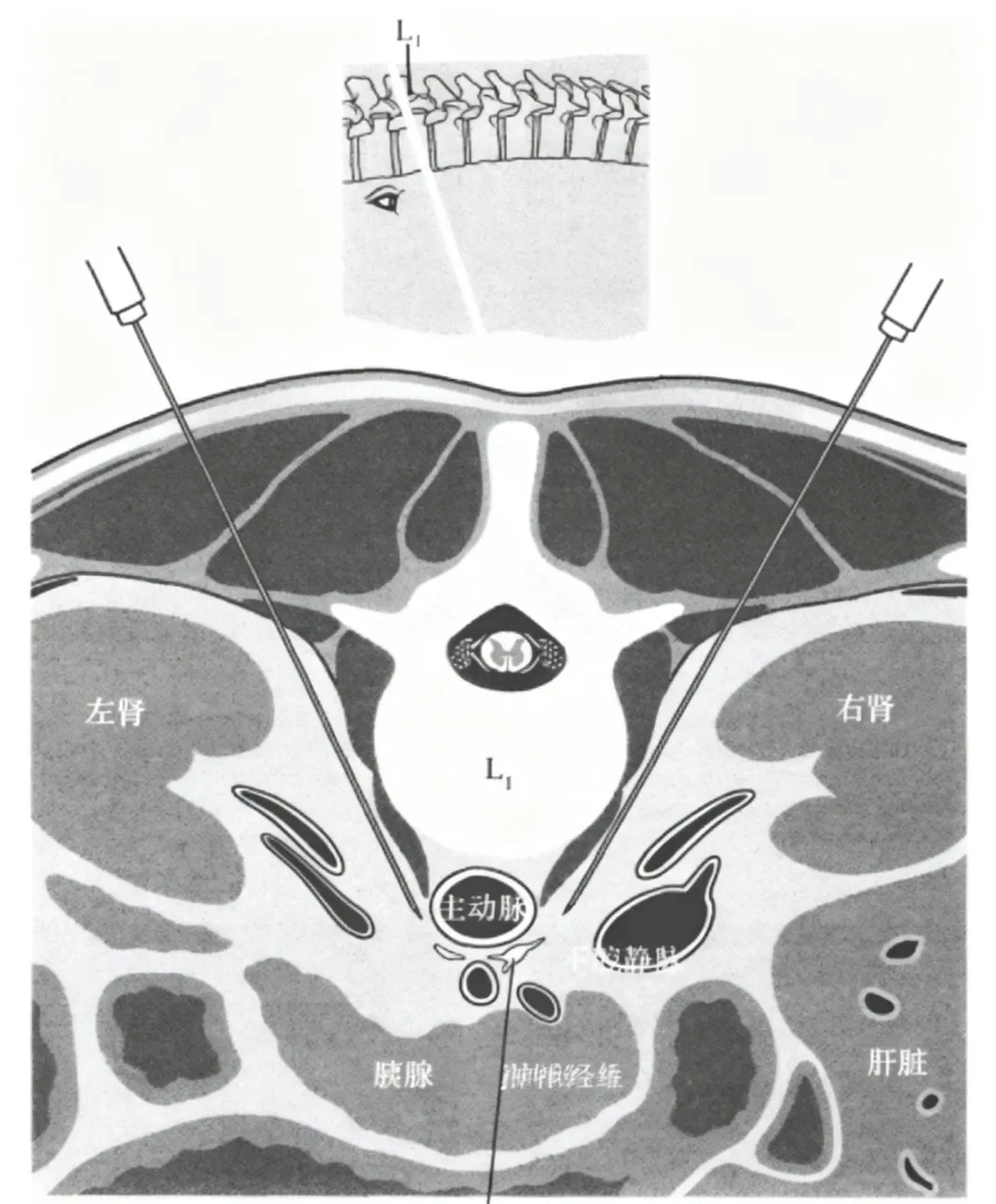
「Images generated by AI, for medical science popularization reference only」
V. Drug Selection
1. Nerve Block: Use a mixture of 0.8%–1% lidocaine combined with 0.25% ropivacaine. Administer 5–10 ml on each side.
2. Nerve Neurolysis: Use >50% ethanol (absolute alcohol) to irreversibly destroy nerve fibers. Before injecting ethanol, first inject a local anesthetic plus contrast agent to confirm satisfactory drug dispersion. Then, inject 10 ml of absolute alcohol on each side.
VI. Preoperative Preparation
1. Complete contrast‑enhanced CT, routine laboratory tests, and other necessary examinations;
2. Sign the informed consent form;
3. Fast for 6 hours and abstain from liquids for 2 hours before the procedure;
4. Establish intravenous access; perform preoperative volume expansion based on the patient's condition;
5. Avoid the use of potent sedatives.
VII. Surgical Operation Procedures
1. Place the patient in the prone position with a cushion under the abdomen. Routinely monitor vital signs, and administer oxygen and sedation as needed.
2. Use CT to localize the T12‑L1 vertebral level, plan the puncture route, sterilize and drape the area, administer local anesthesia, and gradually puncture to reach the target site in the pre‑crural space. The needle tip on the right side should be approximately 2 cm deeper than on the left.
3. After the needle tip is in place, aspirate to confirm no blood or fluid return, then inject contrast agent to confirm the position.
4. For a simple block, directly inject the local anesthetic mixture. For neurolysis, first administer a local anesthetic block, then inject absolute alcohol. Before withdrawing the needle, inject a small amount of normal saline to prevent leakage of the neurolytic agent and damage to normal tissues.
「Images generated by AI, for medical science popularization reference only」
VIII. Postoperative Precautions
1. Efficacy observation: Some patients may experience transient worsening of pain within the first 24 hours after the procedure; symptomatic analgesia can be provided. Pain relief and increased bowel motility are signs of effective treatment.
2. Nursing monitoring: Maintain bed rest for 6 hours. Provide a light liquid diet. Continuously monitor blood pressure, heart rate, and other vital signs, and promptly manage abnormalities such as hypotension.
3. Complications: Mild complications may include hypotension, diarrhea, local pain, or burning pain in the chest/back. Serious complications such as bleeding, organ injury, or nerve injury are rare and can be prevented and managed according to relevant expert consensus.
4. Key points: Pre‑crural space administration is preferred for better efficacy and fewer complications. The extent of drug dispersion is more important than drug concentration. Patients should be clearly informed of the limitations of the treatment.
IX. Classic Surgical Cases
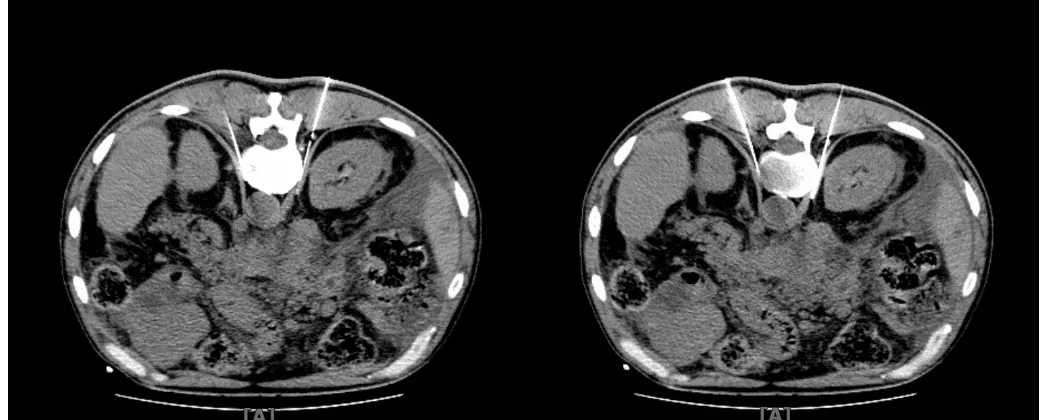
A 60‑year‑old male patient with multiple metastases from a malignant pancreatic tumor experienced long‑term abdominal pain, predominantly on the right side. Before undergoing his first celiac plexus neurolysis procedure, his NRS score was 8; after the procedure, his NRS score dropped to 3.
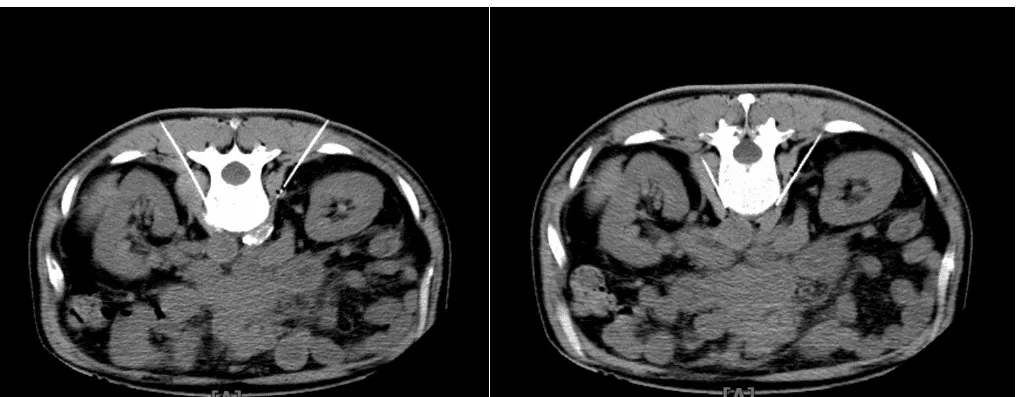
After his first celiac plexus neurolysis, the patient's abdominal pain was significantly relieved, and his constipation improved. He subsequently underwent a second celiac plexus neurolysis procedure. Before the second procedure, his NRS score was 4; after the procedure, it dropped to 1. The patient was satisfied with the treatment outcome.
X. Advantages of CT-guided Technology
CT can clearly delineate abdominal anatomy, tumor extent, and vascular variations, allowing precise planning of the puncture trajectory. It enables real‑time monitoring of needle depth and angle, as well as dynamic observation of drug dispersion, helping to avoid drug leakage and unintentional injury to surrounding tissues. This guidance method offers high precision and can significantly reduce the incidence of surgical complications.
Department of Pain Introduction
Our hospital's Department of Pain Medicine is a specialized unit dedicated to the standardized diagnosis and treatment of various pain disorders. With strong medical expertise and advanced diagnostic and treatment concepts, the department is committed to precisely relieving pain and improving the quality of life for patients suffering from pain conditions.

The department is led by Associate Chief Physician Zhang Depeng, with a medical team rich in clinical experience, solid professional expertise, and years of dedicated focus in the field of pain medicine. The department has a broad scope of practice and specializes in the diagnosis and treatment of various acute and chronic pain conditions, cancer pain arising from different malignant tumors, as well as refractory pain that responds poorly to conventional treatment. The team accurately identifies the causes of pain and develops individualized treatment plans.
Our department actively performs a range of cutting‑edge, minimally invasive analgesic techniques, routinely and expertly carrying out procedures such as intrathecal analgesic pump implantation, neuromodulation electrode implantation, celiac plexus neurolysis, and neuroradiofrequency modulation. With the advantages of minimal trauma, fast recovery, and durable pain relief, these techniques overcome the limitations of traditional conservative treatments, effectively addressing moderate‑to‑severe pain, advanced cancer pain, and complex, refractory pain conditions.
The Department of Pain Medicine consistently upholds the service philosophy of precision diagnosis and treatment, minimally invasive pain relief, and humanistic care. Leveraging mature medical technologies and a comprehensive diagnostic and treatment system, the department provides professional, safe, and efficient one‑stop pain management services for patients suffering from neck, shoulder, low back, and leg pain, neuropathic pain, chronic postoperative pain, and severe pain due to advanced tumors, helping patients break free from pain and regain a comfortable, healthy life.
Consultation and Medical Treatment
Contact Person: Director Zhang Depeng, 15101397118
Medical Address 1: Consulting Room 513, Outpatient Department, Central Campus, Wuwei Academy of Medical Sciences
Medical Address 2: 1st Floor, Building 9, Heavy Ion Campus, Wuwei Academy of Medical Sciences
Author: Zou Ying
Initial Review: Zhang Jie
Secondary Review: Guo Yishan
Third Review: Cai Qinghua