
Transforming for Growth, Innovating through Development
Transforming for Growth, Innovating through Development
Pancreatic cancer is one of the most common malignant tumors in the digestive system and is notoriously known as the "King of Cancers" in the field of oncology. The primary reasons include:
1.Deep Anatomical Location & Concealed Onset
The pancreas is located deep within the body, making pancreatic cancer highly insidious. Routine physical examinations often fail to detect it.
2.Nonspecific Early Symptoms & Misdiagnosis Risk
Early-stage symptoms are usually mild, such as slight abdominal pain, loss of appetite, nausea, and vomiting, which can easily be mistaken for cholecystitis or gastric disorders. By the time the tumor compresses nerves and causes severe pain, the disease has typically progressed to an advanced stage.
3. Limited Treatment Sensitivity & High Surgical Risks
Pancreatic cancer is relatively resistant to radiotherapy and chemotherapy. Surgical resection remains the primary treatment, but the procedure is highly complex, carries significant risks, and is associated with numerous postoperative complications.
4.High Malignancy & Rapid Progression
Pancreatic cancer is extremely aggressive and progresses quickly. Due to the pancreas' proximity to dense networks of nerves, blood vessels, and organs, cancer cells metastasize easily. The resection rate is low, and postoperative recurrence and metastasis rates remain relatively high.
Pancreatic cancer, once diagnosed without the opportunity for radical surgery, has an average survival period of about three to six months. Some patients may undergo radical surgical resection, but the overall five-year survival rate post-surgery does not exceed 5%.
The incidence of this disease is higher in men than in women, with a male-to-female ratio of 1.5–2:1. Men are far more commonly affected than premenopausal women, while the incidence in postmenopausal women is similar to that in men. The primary challenges in diagnosing and treating pancreatic cancer lie in its insidious onset and rapid metastasis.
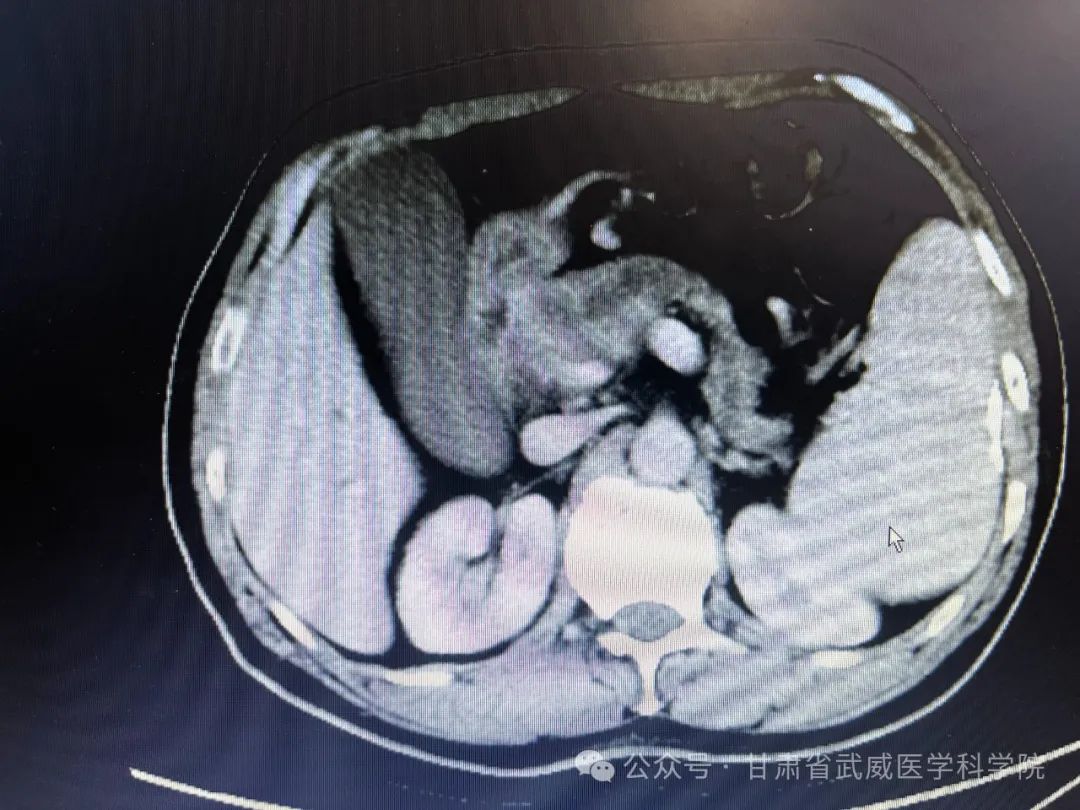
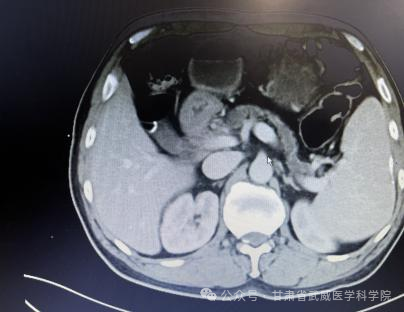
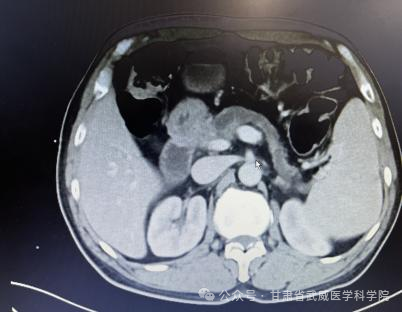
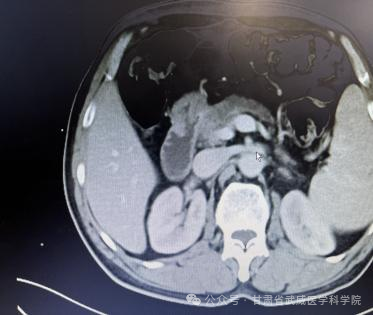
The Abdominal Surgery Department of Wuwei Cancer Hospital, leveraging its strong technical capabilities, recently treated several high-difficulty cases, including hilar cholangiocarcinoma and pancreatic cancer. All surgeries were successfully performed, and the patients recovered smoothly and were discharged. In February 2023, our department admitted a patient with a pancreatic head mass. After careful imaging review by the department director and a full departmental discussion, it was determined that the pancreatic cancer had invaded the portal vein (circumferential involvement exceeding 180°) and the gastroduodenal artery, leaving no opportunity for surgical resection. Following five cycles of systemic intravenous chemotherapy (Gemcitabine 1000 mg/m² + Albumin-bound Paclitaxel 125 mg/m² on D1 and D8), a CT re-evaluation showed significant shrinkage of the pancreatic tumor, creating a gap between the tumor and the main portal vein as well as the gastroduodenal artery. After thorough communication with the patient's family regarding the condition, the patient underwent "radical pancreaticoduodenectomy + I125 seed implantation" in July 2023. The patient has since recovered well, with an overall survival time exceeding one year.
Abdominal CT findings at the time of diagnosis


Post-treatment abdominal CT scan after 5 cycles of chemotherapy
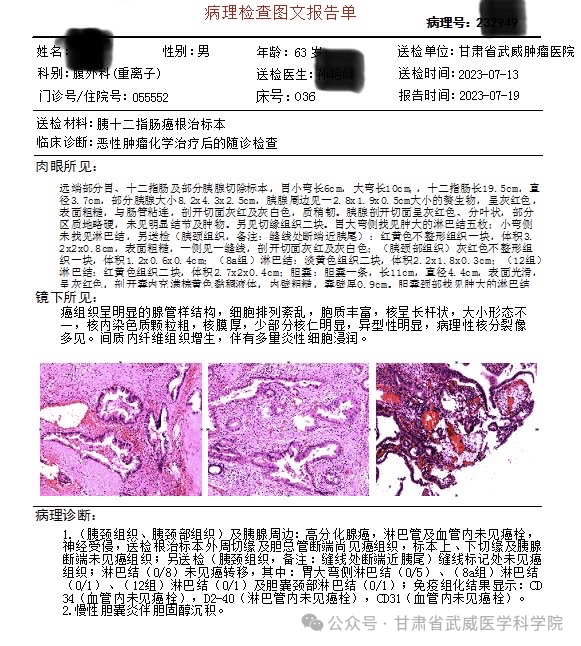
Postoperative pathology report:
- (Pancreatic neck tissue and surrounding pancreas): Well-differentiated adenocarcinoma. No tumor emboli identified in lymphatic or blood vessels (lymphovascular invasion negative). Perineural invasion present.
- Residual carcinoma detected at peripheral resection margin and common bile duct stump.
- Negative for malignancy at superior/inferior resection margins and pancreatic transection margin.
- No tumor found at suture-marked margin (pancreatic neck tissue near tail, noted with surgical thread).
- Lymph node metastasis (0/8):
• Greater curvature of stomach (0/5)
• Group 8a (0/1)
• Group 12 (0/1)
• Gallbladder neck (0/1) - Immunohistochemistry:
CD34 (vascular tumor emboli negative)
D2-40 (lymphatic tumor emboli negative)
CD31 (vascular tumor emboli negative)
2. Chronic cholecystitis with cholesterol deposition.
This patient represents a rare case of advanced pancreatic cancer who achieved successful resection after neoadjuvant conversion therapy with excellent recovery. While we've made progress in treating pancreatic cancer, there remains a long road ahead. Recently, our department has admitted several similar cases who are undergoing standardized neoadjuvant therapy and will undergo scheduled reevaluation for potential surgery. We remain committed to providing surgical solutions through our persistent efforts.
Li Shigong
Department Director

Deputy Chief Physician
Former Director of Hepatobiliary-Pancreatic-Spleen Surgery at Wuwei Academy of Medical and Science Hospital
Current:
- Chief of General Surgery, Wuwei Cancer Hospital
- Director of Abdominal Surgery Department
Education & Affiliations
- MD from Clinical Medicine Department, Lanzhou Medical College
- Associate Professor at Hubei Minzu University
- Standing Committee Member:
• Gastrointestinal Surgery, China Cancer Alliance (Gansu Chapter)
• Liver/Biliary/Pancreatic Tumor Committee, Gansu Medical Doctor Association & Anti-Cancer Association - Vice Chair, Chongqing Surgical Specialization Committee
Advanced Training
- Beijing Anzhen Hospital (Capital Medical University)
- Eastern Hepatobiliary Surgery Hospital (Naval Medical University)
- Ruijin Hospital (Shanghai Jiao Tong University)
Surgical Expertise
Specializes in:
- Open/Laparoscopic/Robotic procedures for GI & hepatopancreatobiliary malignancies
- Routine performance of:
• Laparoscopic radical gastrectomy
• Laparoscopic colorectal cancer resection
• Hepatectomy
• Radical cholecystectomy
• Hilar cholangiocarcinoma resection
• Pancreaticoduodenectomy (Whipple procedure)
Achievements
- 2× Wuwei City Scientific Progress Awards (Second Prize)
- 3 publications in core national medical journals


Department of Abdominal Surgery Overview
Medical Team
- Deputy Chief Physicians: 2
- Attending Physicians: 1
- Resident Physicians: 3
Surgical Expertise
Procedures Performed:
- Open & Laparoscopic Oncologic Surgeries:Radical gastrectomy (gastric cancer)Colectomy/proctectomy (colorectal cancer)Hepatectomy (liver tumors)Distal pancreatectomy with splenectomyMultivisceral resection for metastatic cancers (gastric/colorectal liver metastases)Radical cholecystectomyPancreaticoduodenectomy (Whipple procedure) for pancreatic head/duodenal/bile duct tumorsHilar cholangiocarcinoma resection
- Minimally Invasive General Surgeries:Laparoscopic cholecystectomy (gallstones)Hernia repairOther common general surgical procedures
Contact Information
- Department Phone: +86 935 698 9803
- Key Personnel:
- Li Shigong: +86 150 2592 7869
- Tao Jichun: +86 138 3053 9708
- Sun Yanfeng: +86 138 8455 4011

