
Seek Advancement in Transformation, Pursue Innovation in Development
Seek Advancement in Transformation, Pursue Innovation in Development
Pancreatic cancer is one of the most common and aggressive malignancies of the digestive system, often referred to as the "king of cancers" in oncology. The main reasons for this grim designation include:
(1)Anatomical location: The pancreas resides deep within the abdominal cavity, making early detection extremely challenging during routine physical examinations.
(2)Insidious onset: Early-stage symptoms are typically vague and easily misattributed to benign conditions - mild abdominal pain, loss of appetite, nausea, and vomiting often lead to misdiagnosis as cholecystitis or gastric disorders. By the time neurological symptoms manifest due to nerve compression, the disease has usually progressed to an advanced stage.
(3)Treatment limitations: Pancreatic cancer exhibits relative resistance to radiotherapy and chemotherapy. While surgical resection remains the primary treatment modality, the procedure is technically demanding with high operative risks and frequent postoperative complications.
(4)Aggressive biological behavior: The malignancy demonstrates exceptionally rapid progression. The pancreas' proximity to abundant nerves, blood vessels, and adjacent organs facilitates early metastasis. This results in low resectability rates and high incidences of postoperative recurrence and distant metastasis.
Once pancreatic cancer is diagnosed without the possibility of curative surgical resection, the average survival time is approximately 3 to 6 months. For patients who are eligible for radical surgical resection, the overall 5-year survival rate rarely exceeds 5%.
This disease exhibits a higher incidence in males than females, with a male-to-female ratio of 1.5-2:1. Male patients are significantly more affected than premenopausal women, while the incidence in postmenopausal women approaches that of males. The diagnostic and therapeutic challenges of pancreatic cancer primarily stem from its insidious onset and rapid metastatic progression.
Wuwei Cancer Hospital's Department of Abdominal Surgery, leveraging its robust technical expertise, has recently successfully treated several high-difficulty cases including hilar cholangiocarcinoma and pancreatic cancer, with all patients recovering smoothly and being discharged. In February 2023, our department admitted a patient with a pancreatic head mass. After meticulous imaging review by our department director and comprehensive team discussion, we determined that the pancreatic cancer had invaded the portal vein (circumferential involvement exceeding 180 degrees) and the gastroduodenal artery, rendering surgical resection impossible. The patient underwent five preoperative cycles of systemic intravenous chemotherapy (gemcitabine 1000mg/m2 + nab-paclitaxel 125mg/m2 on days 1 and 8). CT re-evaluation showed significant tumor shrinkage and creation of a measurable space between the pancreatic mass and the portal vein trunk as well as the gastroduodenal artery. After thorough discussion of the prognosis with the patient's family, we performed a "radical pancreatoduodenectomy with I125 seed implantation" in July 2023. The patient has since recovered well, with overall survival exceeding one year.
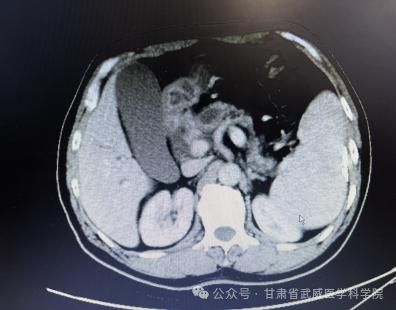
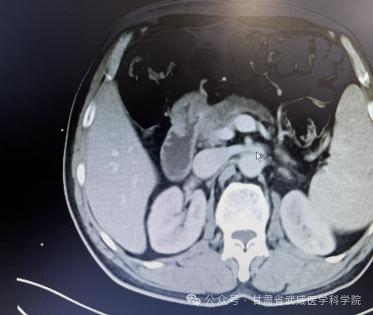
Abdominal CT findings at diagnosis
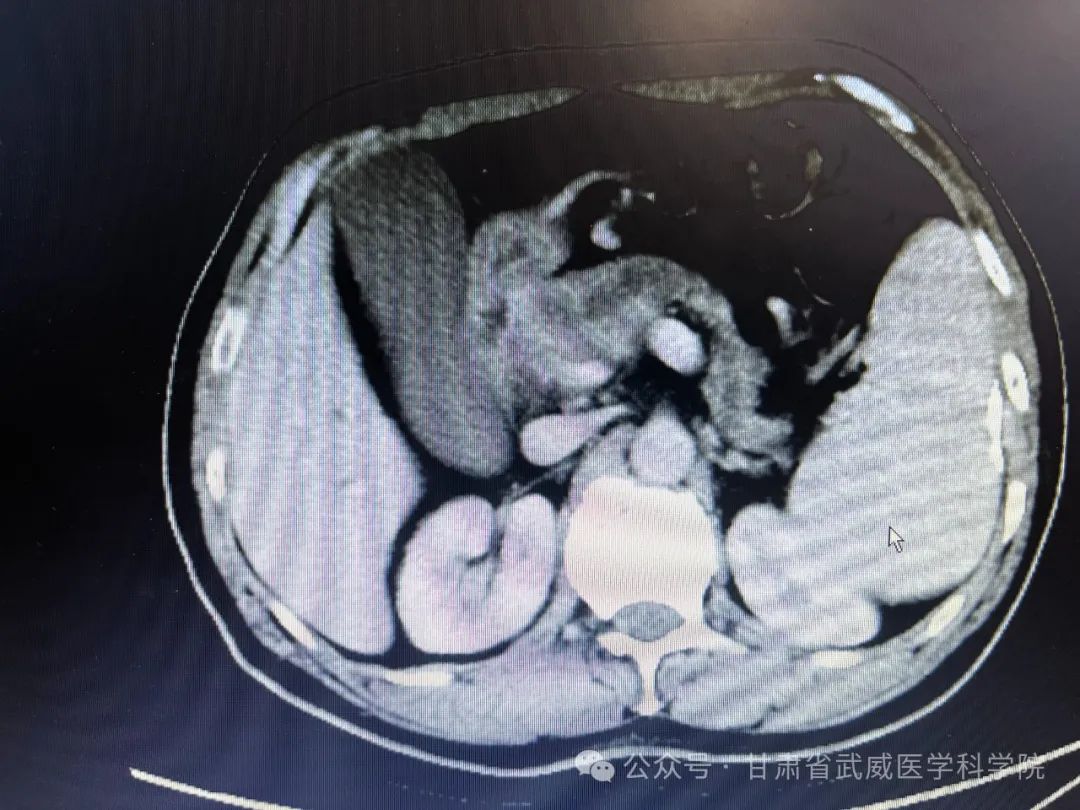

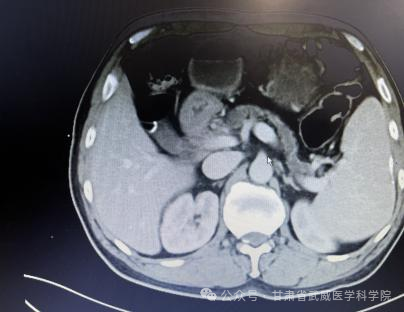
Abdominal CT scan results after 5 cycles of chemotherapy

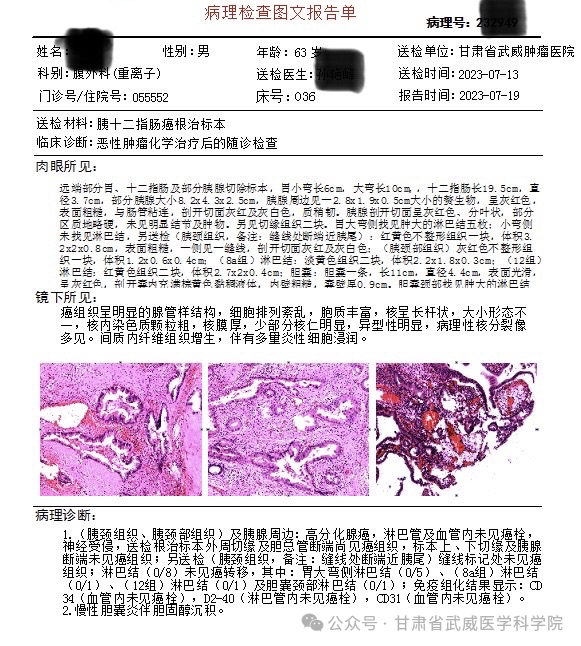
Postoperative pathological findings:
1. Pancreatic neck tissue and peripancreatic tissues: Well-differentiated adenocarcinoma, with no cancer emboli in lymphatic or blood vessels but neural invasion present. Cancerous tissue was observed at the peripheral margin of the radical resection specimen and the common bile duct transection margin, while no cancerous tissue was found at the superior/inferior margins or pancreatic transection margin. Examination of the additionally submitted pancreatic neck tissue (marked with sutures near the pancreatic tail) showed no cancerous tissue at the sutured margin. Lymph nodes (0/8) showed no metastasis, including: greater curvature of stomach lymph nodes (0/5), group 8a lymph nodes (0/1), group 12 lymph nodes (0/1), and cystic duct neck lymph nodes (0/1). Immunohistochemistry results: CD34 (no cancer emboli in vessels), D2-40 (no cancer emboli in lymphatics), CD31 (no cancer emboli in vessels).
2. Chronic cholecystitis with cholesterol deposition.
This patient represents one of the few cases of advanced pancreatic cancer who achieved successful resection after preoperative conversion therapy, with favorable postoperative recovery. While we have made progress in treating pancreatic cancer, there remains a long way to go. Recently, our department has admitted several similar cases of pancreatic cancer. After standardized neoadjuvant therapy, we plan to conduct periodic evaluations to assess their conditions, with the ultimate goal of performing surgical interventions for these patients through our continued efforts.
Discipline Leader Li Shigong

Associate Chief Physician, former Director of the Hepatobiliary, Pancreatic and Splenic Surgery Department at Wuwei Academy of Medical and Science Cancer Hospital, current Director of the General Surgery Department and Abdominal Surgery Department at Wuwei Cancer Hospital. Graduated from the Clinical Medicine Department of Lanzhou Medical College, Associate Professor at Hubei Minzu University. Serves as Executive Committee Member of the Gastrointestinal Surgery Group of Gansu Alliance of China Anti-Cancer Association, Executive Committee Member of the Liver, Biliary and Pancreatic Tumor Committees of Gansu Medical Doctor Association and Gansu Anti-Cancer Association, Deputy Director of the Chongqing Surgical Professional Committee. Completed advanced training at Beijing Anzhen Hospital affiliated to Capital Medical University, Eastern Hepatobiliary Surgery Hospital affiliated to Naval Medical University, and Ruijin Hospital affiliated to Shanghai Jiao Tong University.
Technical expertise: Specializes in traditional open surgery, laparoscopic minimally invasive surgery, and robotic surgery for gastrointestinal, hepatobiliary, pancreatic, and abdominal tumors. Proficient in performing standardized laparoscopic radical gastrectomy, laparoscopic radical colectomy, hepatic tumor resection, radical cholecystectomy, radical hilar cholangiocarcinoma surgery, and complex pancreaticoduodenectomy for duodenal, biliary, and pancreatic tumors. Recipient of 2 Wuwei Municipal Science and Technology Progress Awards (Second Class), with 3 papers published in national core journals.
Introduction to Abdominal Surgery


The department has two associate chief physicians, one attending physician, and three resident physicians.
Department's Technical Expertise
The department's surgical scope includes: traditional open and laparoscopic radical gastrectomy for gastric cancer, radical resection for colon and rectal cancer; hepatic tumor resection, combined splenectomy for pancreatic body-tail tumors; combined organ resection for gastric and colorectal liver metastases; radical cholecystectomy for gallbladder cancer; pancreaticoduodenectomy for pancreatic head tumors, biliary tract tumors, and duodenal tumors; radical resection for hilar cholangiocarcinoma; as well as laparoscopic surgical treatment of common general surgical conditions such as gallbladder stones and hernias.
Contact Information
Department Phone:+86 0935-6989803
Contacts: Li Shigong +86 1502592786, Tao Jichun +86 13830539708, Sun Yanfeng +86 13884554011

