
Taking an Alternative Approach to Relieve Patients' Swallowing Difficulties
Taking an Alternative Approach to Relieve Patients' Swallowing Difficulties
--Percutaneous Endoscopic Gastrostomy/Jejunostomy (PEG/J)
I. Definition and Background
Percutaneous endoscopic gastrostomy (PEG) is a method of tube feeding that involves puncturing the abdominal wall under endoscopic guidance to access the stomach cavity, followed by placement of a gastric or jejunal feeding tube to achieve enteral nutrition and other purposes. It can be used for gastrointestinal drainage, decompression, administration of elemental diets, and bile reinfusion, with high success rates and proven efficacy. PEG was first introduced in 1980 and has gradually replaced traditional surgical gastrostomy, being widely applied to patients who are unable or insufficiently able to eat due to various diseases, providing enteral nutrition support while preserving the absorptive and motor functions of the gastrointestinal tract as much as possible. PEG/J has become the preferred method for long-term tube feeding enteral nutrition due to its simplicity, low complication rate, and good tolerability. Patients with malnutrition caused by various diseases who are unlikely to resume oral intake in the short term or require long-term gastric decompression PEG/J placement may be considered to improve their nutritional status.
II. Indications
1. Before or after radiotherapy or surgery for head and neck tumors;
2. Dysphagia caused by central nervous system injuries;
3. Stroke, traumatic brain injury, or persistent vegetative state;
4. Patients with respiratory dysfunction requiring tracheostomy;
5. Esophageal perforation or anastomotic leakage;
6. Oral intake impairment with normal gastrointestinal function;
7. Patients requiring long-term enteral nutrition support or prolonged gastric decompression.


III. Advantages of Percutaneous Gastrostomy
1. Reduces the risk of gastroesophageal reflux and minimizes nasal and pharyngeal discomfort for patients;
2. Preserves patient appearance and dignity, allowing tube feeding at home;
3. Follows physiological processes—nutrients are absorbed through the intestines into the liver, where they are synthesized and detoxified;
4. Prevents intestinal mucosal atrophy and preserves gut barrier function;
5. Relatively low cost.
Operation Process and Diagram
Procedure for Using a Gastrostomy Tube
Before using a percutaneous endoscopic gastrostomy (PEG) tube, the following procedures must be completed:
Preoperative assessment. Preoperative examinations are required to evaluate whether the patient can tolerate painless gastroscopy.
1. Including complete blood count, coagulation function, liver function, electrolytes, CT scan, and electrocardiogram. Anticoagulant medications must be discontinued at least one week prior to the procedure.
2. Since the stomach is a non-sterile environment, prophylactic antibiotics should be administered 0.5-1 hour before the procedure to prevent local skin infection around the stoma after PEG.
3. The patient's condition must be assessed, and psychological support should be provided to conscious patients. They should be informed about possible postoperative discomforts such as nausea, abdominal pain, and bloating, which can be alleviated by deep breathing. Patients must fast for 8-12 hours before the procedure. Removable dentures should be taken out, and the mouth, teeth, and pharynx should be cleaned.
4. Anesthesia: Before the surgery, the anesthesiologist will communicate with the patient to understand their anesthesia history and possible allergies. Anesthesia will be administered before the procedure to ensure a painless and safe operation.
5. Surgical procedure: The physician will use surgical instruments to create a small incision in the patient's abdomen and insert the PEG tube. The position of the tube must be confirmed to be accurate, and it will be secured to the stomach wall with sutures. After the procedure, the surgical site will be cleaned and treated to prevent infection.
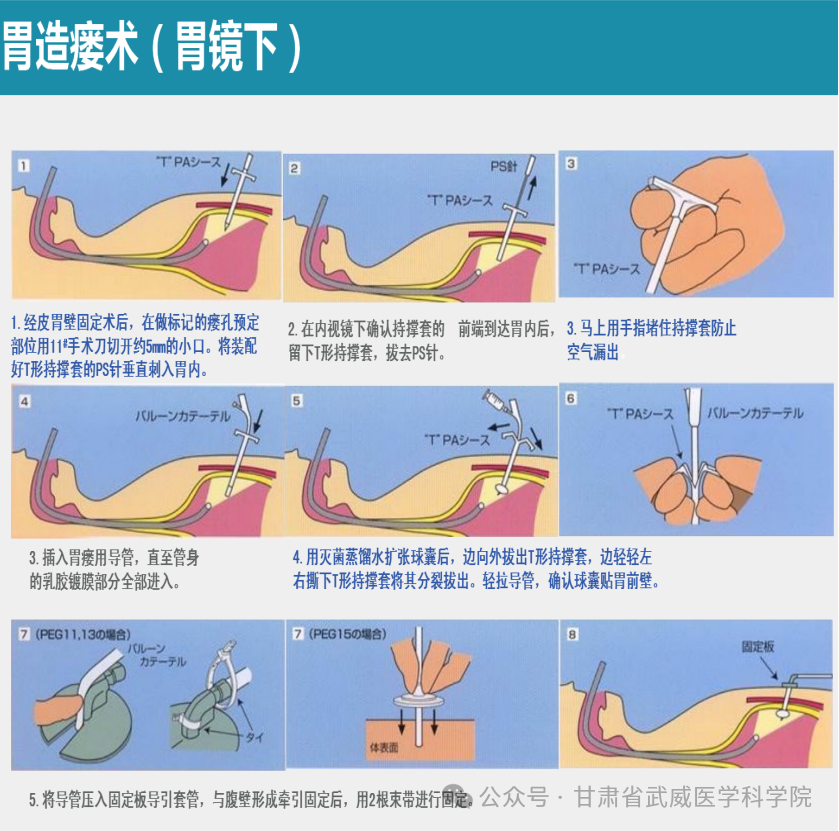
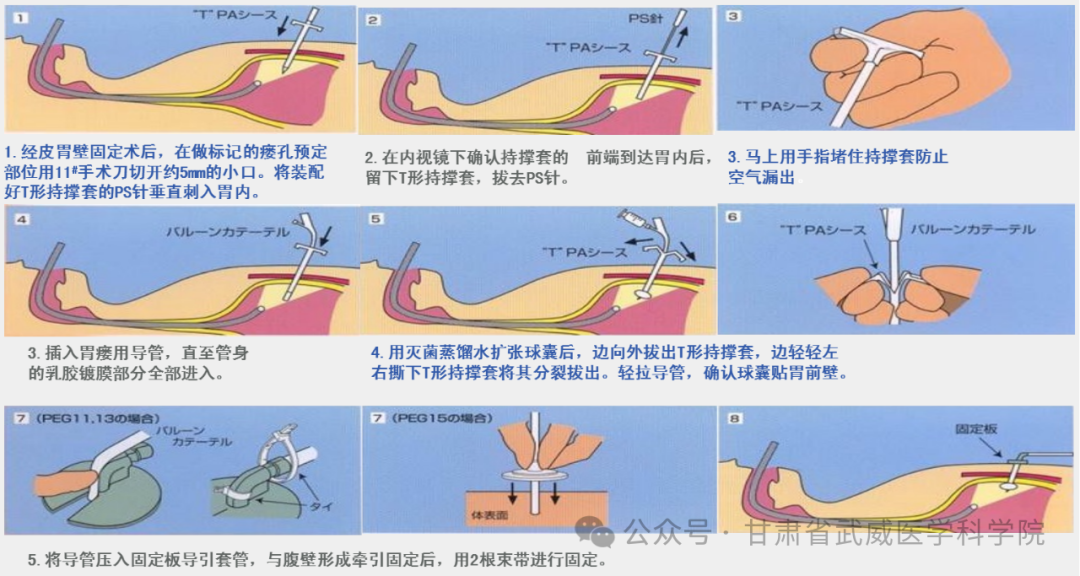
Operation diagram:
Postoperative Care Instructions
Have the patient rest in a semi-recumbent position and reassure them that the procedure was successful. Monitor vital signs and observe for severe chest pain, abdominal pain, hematemesis, or melena, as well as any signs of wound bleeding. Perform daily local disinfection of the stoma site and change the dressing until the stoma has fully formed, while maintaining cleanliness and dryness. Administer antibiotics and acid-suppressing medications as prescribed. Regularly monitor blood biochemistry and liver function.
Stoma Care
1. For the first two weeks postoperatively, disinfect the surrounding skin twice daily with compound iodine (or An iodine), while observing the wound for bleeding, redness, swelling, or discharge, and monitoring the tube depth and any severe pain experienced by the patient. Cut a notch in two large sterile gauze pads (similar to tracheostomy gauze style), with the notch facing downward for the bottom layer and upward for the top layer, then secure them firmly with paper tape. If there is no redness, swelling, or discharge from the wound after one to two weeks postoperatively, reduce dressing changes to once daily. Once the wound has fully healed and a fistula tract has formed, the frequency of dressing changes can be further reduced to 2-3 times per week.
2. Rotate the gastrostomy tube 2-3 times per week (either clockwise or counterclockwise at the base of the tube) to prevent tube occlusion or embedding. Promptly inform the physician and seek medical attention if any of the following symptoms occur: increased drainage, foul odor, redness, swelling, bleeding, localized edema, or severe wound pain.
3. Replace the sterile water in the balloon every 2-3 weeks. Before replacement, first advance the gastrostomy tube 1-2 cm into the stomach, then use a syringe to aspirate the existing sterile water from the balloon. Afterward, inject 10 ml of fresh sterile water into the balloon. Upon completion, disinfect the area again and secure the tube in place.
Dietary Care
1. On the day of surgery, flush the gastrostomy tube with normal saline. The patient should remain nil by mouth for the first 24 hours post-procedure. Enteral feeding via the gastrostomy tube can begin after 24 hours, using either the drip method or push method. The initial daily volume should not exceed 300ml, with gradual increments based on gastric emptying capacity, typically reaching a daily volume of 1500-2000ml.
2. When possible, use nutritionally balanced enteral nutrition formulas such as Nutrison or Fresubin, administered via drip. The infusion rate should not be too rapid, with 500ml solution typically infused over 4-6 hours. In cold weather, use a warming device to prevent hypothermia-induced abdominal pain or diarrhea. For patients with financial constraints, initial feeding may include rice soup, vegetable broth, milk, or fish soup, gradually transitioning to semi-liquid, high-nutrient foods such as mashed vegetables and meats.
3. Administer feedings 4-6 times daily, with each feeding consisting of 200-250ml at a temperature of 38°C-40°C. The infusion rate and volume per feeding should not be excessive. The feeding rate and volume must be strictly adjusted according to gastric emptying status. Before each feeding, aspirate gastric residual volume - if it exceeds 100ml, intolerance should be considered. Pay attention to trace element supplementation and perform regular blood biochemical tests. Oral medications can be dissolved in 30-50ml of water and administered through the tube. Maintain a semi-recumbent position during and for 30-60 minutes after feeding to prevent aspiration; for bedridden patients, elevate the head of the bed by 30 degrees. For patients requiring suctioning, perform suctioning either before feeding or at least one hour after feeding. If coughing or sneezing occurs during feeding, pause immediately and resume only after recovery to prevent aspiration pneumonia. Flush the gastrostomy tube with 20-30ml of warm water before and after each feeding to maintain patency. When oral intake is insufficient, adjust the tube feeding volume accordingly, ensuring tube feeding is administered 1-2 hours after oral intake.
4. If the patient develops diarrhea, check whether the food or equipment is contaminated, or if the food is too cold. Opened food should be used within 24 hours and stored in the refrigerator, then warmed before use. If a confused patient becomes agitated during tube feeding, the food may be too hot.
5. Gastrostomy tube care: Postoperatively, ensure proper fixation of the tube. During each dressing change, check the tube's depth to avoid excessive tightness or looseness. Over-tightening may cause pain and lead to ischemic necrosis of the gastric and abdominal walls, resulting in buried bumper syndrome. If too loose, gastric contents may leak onto the skin due to increased gastric pressure, potentially causing chronic skin irritation, infection, ulceration, non-healing wounds, and fistula formation. For restless or unconscious patients, provide enhanced education to both the patient and family members, and apply wrist restraints if necessary to prevent tube dislodgement.
External guidance
1. Instruct patients to secure the gastrostomy tube to the chest or abdominal wall during rest, activity, or bathing to prevent discomfort or pain caused by swinging or pulling. Particularly after bathing, disinfect the skin around the tube and apply antibiotic ointment.
2. Educate both the patient and family members on feeding procedures, precautions during feeding, and dressing change methods. Advise them to observe the wound condition and tube depth regularly. If any abnormalities occur, immediately stop feeding and seek medical attention. If no abnormalities are present, the tube should be replaced every six months to one year.
3. During each feeding, dirt may accumulate around the stoma, potentially causing skin inflammation. Pay special attention to keeping the area around the stoma clean.
4. After bathing, gently pat the area dry with a towel and allow it to air dry naturally. Apply antibiotic ointment around the stoma if needed.
Instruct family members and the patient on the precautions for tube feeding and the method of dressing changes.
Observe the condition around the stoma and the depth of the gastrostomy tube regularly. Seek medical attention promptly if any abnormalities are detected.
Summary of Efficacy Observation
As a novel enteral nutrition approach, percutaneous endoscopic gastrostomy (PEG) provides reliable nutritional support for patients undergoing treatment. Currently, the Third Department of Gastroenterology in collaboration with the Fifth Department of Radiation Therapy has successfully implemented PEG in over 20 cases of head and neck cancer patients receiving heavy ion therapy. The procedure is performed prior to treatment initiation to ensure adequate nutrition throughout the therapeutic course and recovery period. Clinical observations focus on patients' emotional state, appetite, quality of life, as well as their tolerance and compliance with both the tube placement and treatment regimen.
As an alternative enteral nutrition pathway, PEG demonstrates significant advantages in head and neck cancer radiotherapy. Its application does not increase infection rates, while patients exhibit excellent tolerance and high compliance. This approach effectively restores or improves nutritional status while enhancing quality of life, making it worthy of broader clinical adoption.
The typical radiotherapy course for head and neck cancers lasts 30-50 days, necessitating nutritional support for approximately 1-3 months. For these medium-to-long term patients, selecting an appropriate nutritional access route becomes a critical consideration. The unique challenges of head and neck radiotherapy make nasogastric feeding particularly problematic: it not only causes local mucosal damage with high infection risks, but also leads to increased pain sensitivity in damaged mucosa, exacerbating patient discomfort with the tube. Additionally, nasal tubes significantly impact patients' social activities, resulting in poor compliance and frequent delays in tube placement that compromise nutritional maintenance.
In summary, nutritional deterioration represents a predictable and severe complication during radiotherapy for head and neck malignancies, with dysphagia or swallowing dysfunction being the primary contributing factor. PEG establishes an enteral nutrition pathway with superior safety and patient acceptance, effectively improving nutritional status and providing essential support for subsequent treatments. It stands out as an optimal choice for head and neck cancer patients both before and after radiotherapy.
Introduction to the Department of Gastroenterology, Wuwei Academy of Medical and Science
The Department of Gastroenterology is a key discipline in Gansu Province, a demonstration base for the National Key Public Health Service Project on Early Diagnosis and Treatment of Upper Gastrointestinal Cancers in Rural Areas, a training base for digestive endoscopy professionals accredited by the National Health Commission, a Gansu Provincial Key Laboratory for Gastrointestinal Diseases, the Wuwei Branch of the China Helicobacter pylori Molecular Medicine Center, and the Wuwei Sub-center of the Xijing Biobank, among other prestigious designations.
The department boasts a professional team led by numerous senior experts, including Chief Physician Zhang Zhiyi, a leading talent in Gansu Province's healthcare system and Wuwei City, founder of the Department of Gastroenterology and Director of the Endoscopy Center at Wuwei Medical Science Institute Cancer Hospital; Deputy Director General Nie Peng, Chief Physician (Master of Medicine); Chief Physicians Lin Zhilin, Zhang Wenhong (Master of Medicine); Deputy Director General Zhao Shuguang, Associate Chief Physician (Master of Medicine); Associate Chief Physicians Li Shihua, Liu Jindian (Master of Medicine), and Xie Chunfang, among others.
The Department of Gastroenterology is equipped with over 300 advanced medical devices, including: China's first domestically produced four-arm surgical robot, The fourth PET-CT in Gansu Province and the first PET-CT installed in a prefecture-level hospital in the province, A dynamic 500-slice Gemstone Spectral CT scanner, An Optima 670 64-slice 128-layer spiral CT scanner, The department also houses more than 10 advanced endoscopic surgical systems, such as: STORZ·HD full-HD laparoscopy systems, High-definition 3D thoracoscopes, High-definition 3D fluorescence laparoscopes. Additionally, the department possesses over 30 sophisticated endoscopic instruments, including: Olympus NBI (Narrow Band Imaging) magnifying endoscopes and Ultrasound endoscopes.
Department of Gastroenterology - A New Look




High-tech medical equipment




The Charm of the Heavy Ion Campus





Department of Gastroenterology III Introduction
The Department of Gastroenterology III has a total of 7 physicians (including 2 associate chief physicians, 1 attending physician, and 4 resident physicians) and 9 nurses (comprising 2 senior charge nurses, 3 charge nurses, and 4 registered nurses), with 48 available beds.

The department specializes in diagnosing and treating common and frequently-occurring digestive diseases including gastroesophageal reflux disease, gastritis, peptic ulcers, gastrointestinal bleeding, functional gastrointestinal disorders, and inflammatory bowel disease. It has particular expertise in treating malignant digestive tumors such as esophageal cancer, gastric cancer, pancreatic cancer, liver cancer, cholangiocarcinoma, and colorectal cancer, with special focus on early-stage digestive tract cancers. The department has successfully developed and implemented advanced endoscopic therapeutic techniques including: dilation and stent placement for benign and malignant gastrointestinal strictures, esophageal dilation and stenting, endoscopic repair of esophagotracheal/mediastinal fistulas, sclerotherapy and band ligation for esophageal and gastric varices, gastrostomy, endoscopic treatment of gastric and colonic polyps, endoscopic resection of early-stage digestive cancers (EMR, ESD), endoscopic sclerotherapy and band ligation for esophageal and gastric varices, submucosal tunneling endoscopic resection (STER), peroral endoscopic myotomy (POEM), peroral endoscopic pyloromyotomy (G-POEM), endoscopic retrograde cholangiopancreatography (ERCP), and ultrasound-guided puncture and treatment for biliary and pancreatic system diseases. In addition, the department provides comprehensive cancer care including diagnosis, neoadjuvant chemotherapy, adjuvant chemotherapy, radical chemotherapy for advanced-stage tumors, and multidisciplinary treatment for metastatic cancers, incorporating biological immunotherapy, endocrine therapy, hyperthermic intraperitoneal chemotherapy, and local drug injection therapy for malignant tumors (gastric cancer, esophageal cancer, liver cancer, colorectal cancer, rectal cancer, gallbladder cancer) and lymphomas. The department also offers specialized diagnostic procedures such as small bowel enteroscopy with therapeutic interventions and capsule endoscopy examinations.

Department Director: Zhao Guangyuan
Assistant to the Dean, Discipline Leader
Medical professional profile: As the academic leader and director of the Department of Gastroenterology III, while also serving as assistant hospital president and holding a master's degree in medicine with the title of associate chief physician, graduated from Qinghai University's Gastroenterology program. Completed advanced training at Fukuoka Hospital (Japan), China-Japan Friendship Hospital, Beijing Friendship Hospital, and Wuhan Union Hospital. Specializes in diagnostic and therapeutic interventions for digestive tract tumors, including: esophageal dilation and stent placement, endoscopic repair of esophagotracheal/mediastinal fistulas, sclerotherapy and band ligation for esophageal and gastric varices, gastrostomy, endoscopic treatment of gastric and colonic polyps, endoscopic resection of early-stage digestive cancers (EMR/ESD), endoscopic management of biliary calculi (ERCP), submucosal tumor resection, peroral endoscopic myotomy (POEM) for achalasia, endoscopic ultrasound (EUS) with fine-needle aspiration (EUS-FNA). Expert in comprehensive cancer care for malignancies including gastric, esophageal, liver, colorectal, gallbladder, and pancreatic cancers as well as lymphomas - encompassing diagnostic workup, neoadjuvant/adjuvant chemotherapy, radical chemotherapy for advanced stages, metastatic cancer management, biological immunotherapy, endocrine therapy, molecular targeted therapy, and local drug injection treatments.Published 6 papers in national and provincial medical journals. As principal investigator, completed the Wuwei Science and Technology Bureau research project "Clinical Study of ESD Therapy for Upper Gastrointestinal Submucosal Tumors," which passed expert appraisal in 2014 and won the bureau's second prize in April 2018. Demonstrates exceptional professional diligence by strictly adhering to all medical protocols, conducting meticulous examinations and diagnoses that have significantly reduced misdiagnosis and missed diagnosis rates. Consistently works overtime with perfect attendance throughout the year. Recognized with multiple honors including: Wuwei City Outstanding Physician (2019), Gansu Province Early Cancer Screening Advanced Individual (2019), Wuwei Health System Outstanding Communist Party Member (2021).

Contact Information
Contact number: Zhao Guangyuan: 13884588383 Yang Dechang: 18393155431
Address: Building 3, 3rd floor, Heavy Ion Center of Gansu Wuwei Academy of Medical and Science Cancer Hospital

