
【Expert Q&A】Let’s Explore the Most Common Stomach Disease: Acute Gastritis
【Expert Q&A】Let’s Explore the Most Common Stomach Disease: Acute Gastritis
The Most Common Stomach Disease
Acute Gastritis
Autumn, as a season prone to acute gastritis, often sees its triggers closely linked to poor dietary habits and the consumption of unhealthy foods. These improper intakes may provide opportunities for bacteria or viruses to take hold, silently invading the gastrointestinal tract and subsequently triggering a range of uncomfortable symptoms: sharp, gnawing stomach pain; elevated body temperature accompanied by fever; persistent diarrhea; and in more severe cases, many patients also face daunting challenges such as ongoing nausea, frequent vomiting, and even dehydration.
Today, we have invited Director Zhao Guangyuan from the Third Department of Gastroenterology at Wuwei Academy of Medical Sciences Cancer Hospital to join us in a thorough exploration of acute gastritis, working together to safeguard gastrointestinal health throughout this season.

Zhao Guangyuan, Deputy Chief Physician
• Assistant President, Director of the Third Department of Gastroenterology, Deputy Chief Physician, Master of Medicine.
• In 2017, studied diagnostic and treatment techniques for digestive system diseases in Fukuoka, Japan. After returning from overseas studies, has been engaged in clinical digestive treatment work.
• Pursued further training at China-Japan Friendship Hospital, Beijing Friendship Hospital, and Wuhan Union Hospital.
• Has been engaged in clinical and research work on digestive tract diseases and digestive endoscopy for 20 years, specializing in the examination and treatment of digestive tract tumors.
• Has published 6 papers in national and provincial medical journals. Served as the first principal investigator to complete the scientific research project of the Wuwei Science and Technology Bureau: "Clinical Study on ESD Treatment for Submucosal Tumors of the Upper Digestive Tract," which won the Second Prize from the Wuwei Science and Technology Bureau.
• Has received honorary titles such as "Advanced Individual in Early Cancer Screening in Gansu Province," "Outstanding Physician of Wuwei City," and "Outstanding Communist Party Member in the Health System of Wuwei City."
Editor: Director Zhao, could you please explain to everyone what acute gastritis is?
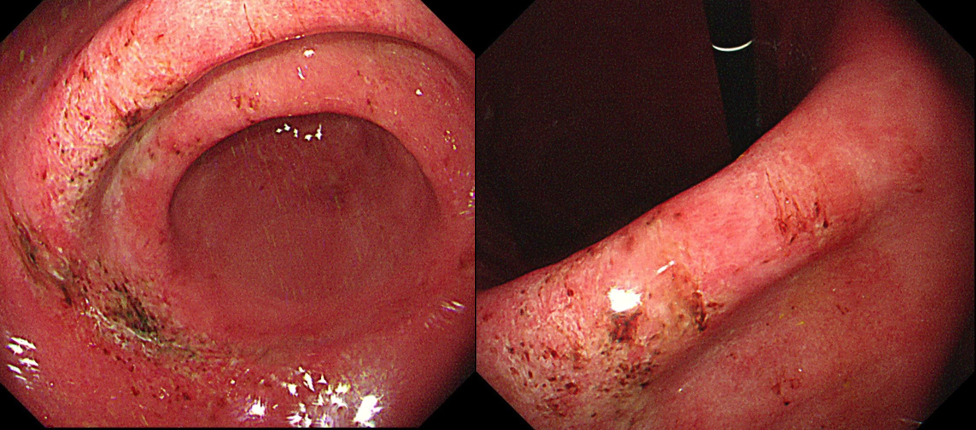
Director Zhao Guangyuan: Acute gastritis, as an acute inflammation of the gastric mucosa, has a complex etiology that encompasses both external irritants and internal factors. Under detailed gastroscopic observation, this condition manifests typical signs such as congestion, edema, erosion, and even hemorrhage of the gastric mucosa, along with transient pathological changes like associated inflammatory exudate. Based on specific manifestations of the lesions, acute gastritis is subdivided into four major categories: acute simple gastritis, acute erosive gastritis, acute suppurative gastritis, and acute corrosive gastritis—among which the first two are more common clinically. It is particularly worth mentioning that acute simple gastritis, due to its high incidence, has become one of the most frequently encountered digestive system diseases in clinical practice.
Acute Erosive Gastritis
Dubbed a gastric inflammation that "causes bleeding," it is fortunate that as long as its precipitating factors are promptly identified and eliminated, the prognosis is generally favorable.
Acute Corrosive Gastritis
This condition is often closely linked to a history of accidental ingestion of strong acids or alkalis. Patients endure unbearable, severe abdominal pain. In such scenarios, early, standardized emergency measures act as a lifeline, effectively ensuring a good prognosis. Conversely, if treatment is delayed, serious complications such as gastric perforation or peritonitis may emerge, threatening the patient’s life.
Acute Suppurative Gastritis
Rooted in invasion by pyogenic bacteria, this type of gastritis often occurs as a consequence of other abdominal diseases. Beyond suffering from chills and high fever, patients must also be alert to the sudden onset of two major complications: acute peritonitis and septic shock.
Acute Gastritis
As a clinical condition that strikes abruptly, its rapid onset often presents first with upper abdominal symptoms. Symptoms vary in severity: milder cases may involve only upper abdominal discomfort, postprandial fullness, accompanied by belching, acid reflux, reduced appetite, or even diarrhea; severe cases, however, may face critical challenges such as hematemesis (vomiting blood), melena (black, tarry stools), dehydration, acidosis, or even fall into a state of shock. In such instances, every minute counts, and immediate medical attention is essential.
Editor: Director Zhao, could you please tell us what the causes of acute gastritis are?
Director Zhao Guangyuan: The main causes of acute gastritis include drug irritation, excessive alcohol consumption, bacterial infection, food poisoning, physical injury, chemical injury, stress factors, and local insufficient blood supply, among others. These factors, whether acting alone or in combination, may all lead to acute inflammation of the gastric mucosa.
01
Acute infection (bacterial and its toxins)
Ingestion of food contaminated with pathogens such as Salmonella, Vibrio parahaemolyticus, Staphylococcus aureus, and enteroviruses—for example, crabs, snails, leftover rice, and dishes—can trigger acute gastritis within a few hours.
02
Medications
The most common culprits are nonsteroidal anti-inflammatory drugs (NSAIDs), such as aspirin, indomethacin, ibuprofen, loxoprofen, diclofenac sodium sustained-release tablets, and others. These medications reduce prostaglandin synthesis in the body, thereby weakening the protective capacity of the gastric mucosa. Other drugs that may adversely affect the stomach include adrenocortical hormones (e.g., prednisone, methylprednisolone), anticoagulants, anti-thrombotic agents, and anti-tumor drugs, among others.
03
Poor dietary habits
Unrestrained eating—including excessive intake of raw or cold, overly hot, or coarse foods—along with frequent consumption of irritating beverages such as strong tea, coffee, and strong spirits, can all directly irritate the gastric mucosa, damage its protective barrier, and thereby induce adverse reactions such as congestion, edema, erosion, and even hemorrhage of the gastric mucosa.
04
Acute stress
When the body is subjected to an acute stress state—such as extreme conditions including major trauma, extensive burns, or severe infection—it triggers spastic contractions in the blood vessels of the gastric mucosa. This leads to hypoxia (insufficient oxygen) and ischemia (reduced blood flow) in the gastric mucosal area, thereby causing damage to the gastric mucosa.
05
Other Factors
Under extreme conditions—such as the corrosive effects of strong acids or alkalis, bile reflux, and other adverse factors—severe damage can be inflicted on the stomach. Additionally, improper use of medications and stress responses often manifest as prominent symptoms of gastrointestinal bleeding, such as melena (black, tarry stools) and hematemesis (vomiting blood). When bleeding volume increases sharply, these symptoms may further lead to severe consequences such as hypotension and even shock.
On the other hand, food poisoning is often closely associated with acute enteritis. It is not only accompanied by frequent diarrhea but may also lead to dehydration. In severe cases, it may induce conditions such as hypotension. Furthermore, corrosive and infectious gastritis present with more severe clinical manifestations. Patients often experience severe upper abdominal pain, accompanied by systemic symptoms such as frequent vomiting, chills, and high fever, posing a significant threat to their health.
Editor: Director Zhao, could you please tell us what examinations are needed to diagnose acute gastritis?
Director Zhao Guangyuan: During diagnosis, we usually comprehensively consider the patient's medical history, clinical manifestations, and a series of relevant symptoms. Specifically, if a patient has an acute onset accompanied by upper abdominal pain and discomfort, as well as typical dyspeptic symptoms such as nausea, vomiting, and loss of appetite, these are all important reference points in our diagnostic process. Below are three examinations I have compiled for everyone's reference.
Complete Blood Count (CBC) Test
An increase in white blood cell count is closely associated with infection. As a core indicator of inflammatory response, it significantly signals enhanced inflammatory activity within the body. When the percentage of neutrophils is elevated, this typically serves as a strong indication of bacterial infection in the patient, providing critical clues for clinical determination of the type of infection.
Furthermore, if a progressive decline in hemoglobin levels is observed alongside an abnormally high hematocrit, this combination suggests that the patient may be in a state of severe blood concentration, indicating that the body is approaching or has reached a critical point of dehydration. These hematological changes not only provide important evidence for assessing the patient's fluid balance but also guide timely diagnosis and treatment of acute gastritis, assisting physicians in formulating more precise treatment strategies.
Stool Routine Test
Using the fecal occult blood test (FOBT)—a sensitive and effective detection method—we can accurately assess whether there is bleeding in the digestive tract. By detecting trace amounts of blood components in feces that are difficult to observe with the naked eye, this test provides clinical information about gastrointestinal bleeding, making it an indispensable part of digestive tract health screening and disease diagnosis.
Gastroscopy
Gastroscopy is typically performed within 24 to 48 hours after the onset of symptoms and is a key method for confirming acute gastritis. This procedure allows for direct and detailed observation of the location and extent of gastric mucosal lesions, as well as precise identification of the specific causes of bleeding. If gastroscopic findings reveal widespread congestion, edema, and exudation of the gastric mucosa, along with spotty hemorrhage, multiple erosions (which are diffusely distributed), hemorrhagic foci, or even superficial ulcers, these strongly indicate that the patient has acute gastritis. This diagnostic method is not only rapid and accurate but also provides a solid basis for subsequent targeted treatment.
Additionally, during the diagnostic process, it is essential to meticulously perform a differential diagnosis of acute gastritis with a range of related diseases to ensure the accuracy of the diagnosis. These diseases include but are not limited to peptic ulcers, acute pancreatitis, cholecystitis, cholelithiasis, and acute appendicitis. Through comprehensive clinical evaluation, detailed medical history inquiry, necessary examinations, and imaging studies, we can more precisely differentiate these conditions and develop more personalized and targeted treatment plans for patients.
Editor: Director Zhao, may I ask how acute gastritis should be treated?
Director Zhao Guangyuan: The treatment strategy for acute gastritis encompasses four core aspects: eliminating the underlying causes, strengthening gastric mucosal protection, adjusting to an appropriate diet, and implementing precise symptomatic management. The primary step is to immediately discontinue the intake or exposure to all foods and medications that may irritate the stomach. For patients with significantly aggravated symptoms, acid-suppressing medications and potent mucosal protectants should also be administered to rapidly alleviate discomfort. During treatment, strictly adhering to medical advice is crucial, including taking antispasmodic measures to relieve spasmodic stomach pain, performing timely fluid replacement to correct fluid and electrolyte imbalances, applying antiemetic treatment to alleviate nausea and vomiting, and conducting necessary anti-inflammatory therapy to control the progression of inflammation. Of particular importance, if signs of bleeding are detected, endoscopic hemostatic measures should be initiated immediately to rapidly and effectively control the bleeding.
Summary
After the effective elimination of the underlying causes, acute gastritis can generally self-heal within a short period. During this time, patients are advised to engage in appropriate bed rest, which not only aids physical recovery but also facilitates psychological adjustment and alleviates anxiety. Meanwhile, dietary hygiene should be a key focus, and any actions that may exacerbate gastric burden or irritate the gastric mucosa—such as overeating—must be avoided.
In terms of diet, light, easily digestible semi-liquid foods (e.g., porridge and soups) are recommended. These foods meet the body’s nutritional needs without excessively irritating the gastric mucosa. Conversely, fatty fish or meat cooked by deep-frying, pan-frying, smoking, or curing, as well as high-fiber vegetables and fruits, strongly stimulating foods, and pungent condiments should all be avoided to prevent exacerbating the condition or delaying recovery.
In summary, for patients with acute gastritis, good lifestyle habits and reasonable dietary arrangements are equally crucial in addition to necessary medical interventions. Through the comprehensive application of these measures, we can more effectively promote the improvement of the condition and the recovery of the body.
Department of Gastroenterology, Wuwei Cancer Hospital, Gansu Province
Department of Gastroenterology
The Department of Gastroenterology is a Key Discipline of Gansu Province, a Demonstration Base for Early Diagnosis and Early Treatment of Upper Gastrointestinal Cancer under the National Major Public Health Service Program (Rural Cancer Early Diagnosis and Early Treatment Program), a Training Base for Endoscopic Professional Technology in Gastroenterology (authorized by the former National Health and Family Planning Commission), a Gansu Provincial Key Laboratory of Gastroenterology, a Wuwei Sub-center of China Helicobacter pylori Molecular Medicine Center, and a Wuwei Sub-bank of Xijing Biobank, among other prestigious designations.
The department boasts a professional team led by a large number of senior experts, including:
•Zhang Zhiyi, Chief Physician, Founder of the Department of Gastroenterology at Wuwei Academy of Medical Sciences and Oncology Hospital, Director of the Gastroscopy Center, and Leading Talent in Gansu’s Health System;
•Nie Peng, Chief Physician (Master of Medicine), Deputy President;
•Lu Linzhi, Chief Physician;
•Zhang Wenhong, Chief Physician (Master of Medicine);
•Zhao Guangyuan, Deputy Chief Physician (Master of Medicine);
•Li Shihua, Deputy Chief Physician;
•Liu Jindian, Deputy Chief Physician (Master of Medicine);
•Xie Chunfang, Deputy Chief Physician;and other distinguished professionals with senior academic titles.
The department is equipped with over 300 pieces of advanced medical equipment, including:
•The first domestically produced four-arm surgical robot in China;
•The fourth PET-CT in Gansu Province and the first PET-CT among prefecture-level hospitals in the province;
•Dynamic 500-slice Gemstone Spectral CT;
•Optima 670 64-slice 128-layer spiral CT;Over 10 types of endoscopic surgical instruments, such as STORZ HD full-HD laparoscopes, high-definition 3D thoracoscopes, and high-definition 3D fluorescent laparoscopes;Over 30 endoscopic devices, including Olympus NBI magnifying endoscopes and endoscopic ultrasound (EUS) systems.
Preliminary Review: Zhang Jie
Final Review: Ma Shuqian