
Lighting Hope: Cervical Cancer Radiotherapy Explained
Illuminating Hope: A Science Popularization on Radiotherapy for Cervical Cancer
1. What is Curative Radiotherapy?
Curative radiotherapy refers to a form of radiation therapy aimed at completely eradicating the tumor and achieving disease eradication. It is typically used for cervical cancer patients who are inoperable or at high operative risk, especially those in the locally advanced stages (e.g., IIB-IVA).
Curative radiotherapy is often combined with chemotherapy (i.e., concurrent chemoradiation), which can significantly enhance treatment efficacy.
2. Applicable Population
1. Clinical Staging:
Stage IIB and above (tumor invades parametrium or lower 1/3 of vagina).
Stage IVA (tumor invades bladder/rectal mucosa).
Some Stage IB3-IIA2 tumors that are large or have high-risk factors (e.g., lymph node metastasis).
2. Non-surgical Candidates
Patients with severe cardiopulmonary diseases, advanced age, or other surgical contraindications.
Tumors in special locations or with extensive invasion, making complete surgical resection difficult.
3. Standard Curative Radiotherapy Protocol
1. Combination of radiotherapy techniques
Definitive radiotherapy requires the combination of external beam radiotherapy (EBRT) and brachytherapy, which synergize to enhance efficacy:
External beam radiotherapy: covers the primary cervical lesion, parametrial tissues, and regional lymph nodes.
Recommended techniques: intensity-modulated radiotherapy (IMRT) or volumetric-modulated arc therapy (VMAT) to precisely protect the rectum, bladder, and small intestine.
Dose: 45-50 Gy (delivered in 25-28 fractions, once daily).
Brachytherapy: delivers high-dose radiation directly to the cervical tumor.
Dose: 28-35 Gy (delivered in 3-5 fractions, typically once or twice weekly).
The total equivalent biological dose (EQD2) must be ≥80-85 Gy (a critical indicator affecting cure rates).
2. Concurrent Chemotherapy
Purpose: To enhance radiosensitivity and eliminate micrometastases.
Common regimens: Cisplatin monotherapy (40 mg/m², once weekly) or cisplatin plus 5-FU (every 3 weeks).
Note: Chemotherapy must be administered on the day of radiotherapy or within 24 hours before or after.
4. Treatment Process (Taking Stage IIB as an Example)
1.Pretreatment Evaluation
Imaging assessment: Pelvic MRI (to evaluate tumor extent) + PET-CT (to rule out distant metastases).
Simulation and planning: CT simulation for positioning and creation of individualized radiotherapy plan.
2. External Beam Radiotherapy Phase
Daily sessions, 5 days per week, lasting approximately 5 weeks.
3. Brachytherapy Phase
Initiated within 1-2 weeks after completion of EBRT, usually completed in 3-5 fractions.
4. Concurrent Chemotherapy
Weekly cisplatin chemotherapy administered synchronously with EBRT.
5. Treatment Efficacy and Prognosis
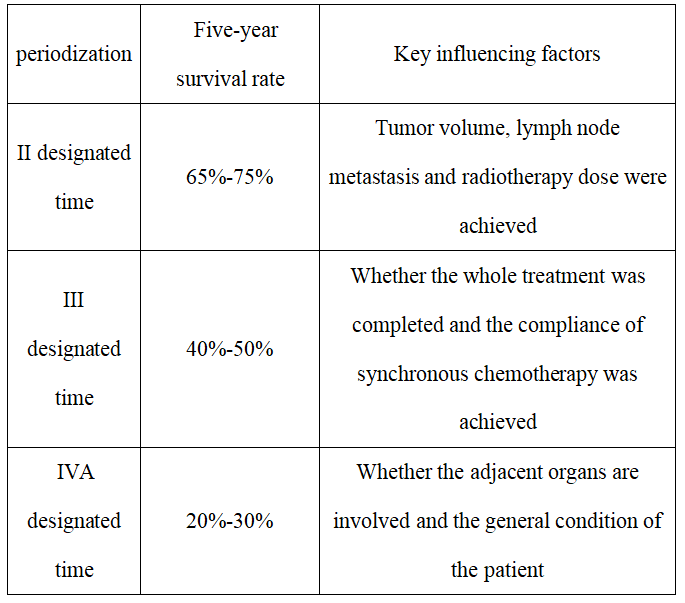
Note: The efficacy of definitive radiotherapy is closely related to the total radiation dose and the standardization of concurrent chemotherapy.
6. Common Side Effects and Management
1. Acute reactions
Radiation enteritis: diarrhea, abdominal pain → low-residue diet + smectite.
Bone marrow suppression: leukopenia/thrombocytopenia → granulocyte colony-stimulating factor or blood transfusion support.
Radiation cystitis: urinary frequency, hematuria → increased fluid intake, anti-inflammatory treatment if necessary.
2. Long-term complications
Vaginal stenosis/adhesion: vaginal dilator use starting 3 months post-radiotherapy.
Rectovaginal/vesicovaginal fistula (rare): requires surgical repair.
Ovarian failure: premenopausal women should consult hormone replacement therapy in advance.
7. Patient Precautions
1. During Treatment
Nutritional support: High-protein, high-vitamin diet; avoid spicy and gas-producing foods (e.g., legumes).
Skin protection: Keep irradiated areas dry; avoid irritating skincare products.
Regular blood tests: Monitor white blood cell and platelet levels (at least once weekly).
2. Post-Treatment Follow-Up
Years 1-2: Pelvic MRI and HPV testing every 3 months.
Years 3-5: Every 6 months, focusing on long-term complications.
3. Lifestyle
Quit smoking and alcohol; engage in moderate exercise (e.g., yoga, walking) to promote pelvic blood circulation.
Psychological counseling: Radiation therapy is prolonged; maintaining a positive mindset is essential.
8. Frequently Asked Questions
Q: What if the tumor doesn't completely disappear after definitive radiotherapy?
A: Additional radiotherapy or surgery may need to be considered, but risks must be carefully weighed.
Q: Will HPV turn negative after radiotherapy?
A: 70%-80% of patients achieve HPV seroconversion post-treatment; persistent positivity warrants close monitoring for recurrence.
Q: How soon can sexual activity resume after radiotherapy?
A: It's recommended to wait 2-3 months post-treatment to allow vaginal mucosal healing, with the use of lubricants to minimize friction.
Definitive radiotherapy remains the cornerstone treatment for locally advanced cervical cancer. By combining precise radiotherapy techniques with chemotherapy, significant survival benefits can be achieved. Patients must strictly adhere to the treatment plan while paying attention to long-term survivorship care. Thorough pre-treatment consultation with physicians is essential to develop individualized treatment strategies.
Department Introduction
The Radiotherapy Department IV specializes in photon and carbon ion therapy for gynecologic and breast malignancies, including cervical cancer, endometrial cancer, vaginal cancer, vulvar cancer, ovarian cancer, and breast cancer. The department provides comprehensive treatment modalities such as definitive radiotherapy, neoadjuvant radiotherapy before surgery, adjuvant radiotherapy after surgery, chemotherapy, immunotherapy, targeted therapy, endocrine therapy, and their combinations. The department consists of 13 medical staff members, including 2 associate senior physicians, 1 attending physician, and 3 resident physicians. Department members have received advanced training at Tianjin Cancer Hospital, Beijing Cancer Hospital, PLA General Hospital (301 Hospital), Peking University Third Hospital, Shanghai Proton and Heavy Ion Hospital, and Sichuan Cancer Hospital.
Department Director Dang Youquan, Associate Chief Physician, has 24 years of experience in oncology radiotherapy. She has received advanced training at multiple renowned top-tier hospitals nationwide and possesses extensive expertise in radiotherapy and comprehensive treatment for gynecologic and breast cancers. Currently, she serves as a committee member of the Ion Radiotherapy Branch of the Chinese Medical Equipment Association, executive director of the Western Oncology Specialty Alliance, standing committee member of the Gansu Provincial Anti-Cancer Association's Brachytherapy Professional Committee, member of the Gansu Provincial Geriatric Medical Association's Radiation Oncology Professional Committee, member of the Gansu Provincial Nutrition Society's Oncology Nutrition Branch, and part-time instructor at Wuwei Vocational College. The department regularly invites Professor Jörg Hauffe from the Munich Proton and Heavy Ion Center in Germany, Professor Hirohiko Tsujii - known as the "world's foremost expert in heavy ion tumor therapy" from Japan, and Professor Yee-Min Jen, former chairman of the Taiwan Regional Oncology Radiotherapy Committee, for regular ward rounds and professional guidance. The department has long been under the clinical, research, and teaching guidance of Professor Liu Zi, chairman of the Gynecologic Oncology Professional Committee at the First Affiliated Hospital of Xi'an Jiaotong University, and Professor Li Sha, chief physician of the Radiotherapy Department at the PLA Joint Logistics Support Force 940th Hospital. The department has completed 5 provincial and municipal research projects, published over 10 academic papers, and obtained 3 invention patents. Over the years, its effective comprehensive cancer treatment approach has achieved excellent clinical outcomes, earning widespread acclaim from patients, peers, and society.


