
Guarding the Vital Center: Precision Intervention After a Ruptured Middle Cerebral Artery Aneurysm
Guarding the Vital Center: Precision Intervention After a Ruptured Middle Cerebral Artery Aneurysm
In emergency neurological conditions, time is often measured in seconds—after a brain aneurysm ruptures, every minute of delay can mean irreversible neurological damage. Recently, the interventional team at our Neurological Medical Center once again successfully performed emergency interventional treatment for a ruptured aneurysm. From diagnosis to catheter lab surgery, the process was seamless, further enhancing the center's technical expertise in minimally invasive interventional treatment for emergency cerebrovascular diseases and its multidisciplinary collaboration capabilities.
Case Review
Patient: Male, 61 years old.
Chief Complaint: Sudden loss of consciousness for 30 minutes.
The patient experienced a sudden loss of consciousness during activity, accompanied by a spasmodic flexion posture of both upper limbs. He regained consciousness spontaneously after 30 minutes. Upon emergency admission, his mental state had cleared, and physical examination revealed no significant neurological deficits.
This clinical presentation of "seeming improvement" could, however, be a dangerous signal—silent subarachnoid hemorrhage.
Image Revealed
Head CT and CTA:
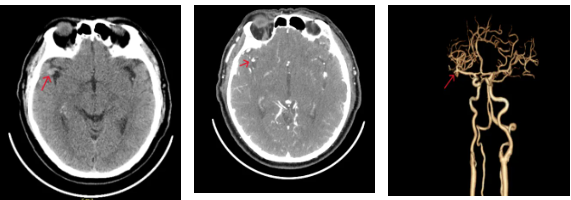
A slightly hyperdense nodule at the origin of the M2 segment of the right middle cerebral artery
Cranial MRI:
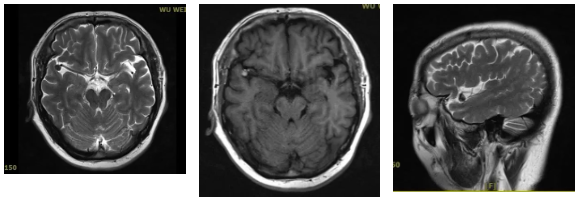
An abnormal signal nodule at the origin of the M2 segment of the right middle cerebral artery, considered to be an aneurysm
Procedure Record
1. Preoperative evaluation, baseline angiography
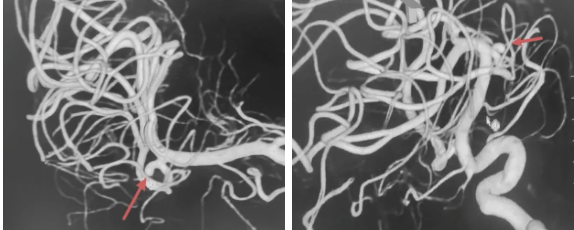
DSA 3D reconstruction shows: an aneurysm is visible at the M2 bifurcation of the middle cerebral artery, and the aneurysm body is irregular
2. Scheme determination and strategy planning

The M2 segment of the middle cerebral artery, known as the "vital junction" of cerebral blood vessels, is an important perforator blood supply area after bifurcation. Traditional craniotomy for clipping involves significant trauma and difficult exposure, with an increased risk of cognitive dysfunction following brain tissue retraction. Furthermore, M2 segment aneurysms are often wide-necked or located at bifurcations, making them prone to recurrence with simple coiling. Therefore, after a comprehensive evaluation of the aneurysm's location and neck width, the surgical plan was determined to be "Atlas stent implantation plus aneurysm coil embolization."
3. Pathway construction, catheter placement
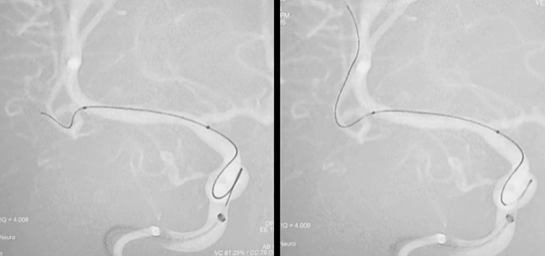
Micro-guidewire super-selection and stent catheter placement
4. Dense packing, stable framing
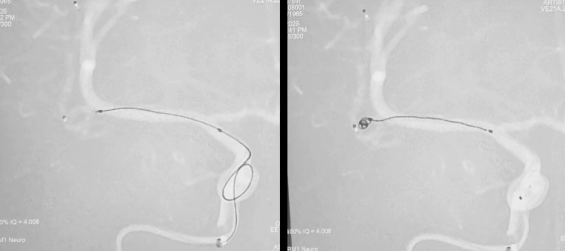
The embolization catheter is in place, and the coils are gradually packed
5. Stent deployment, precise wall apposition
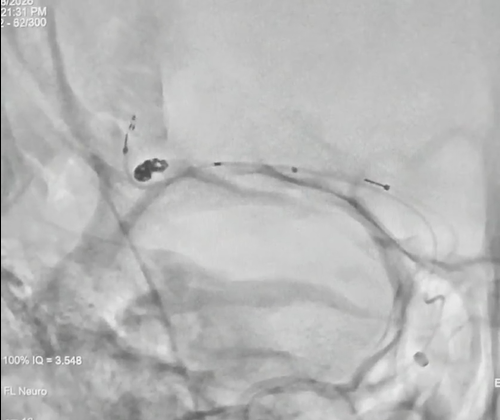
Stent release
6. Alert lifted, returning to daily life
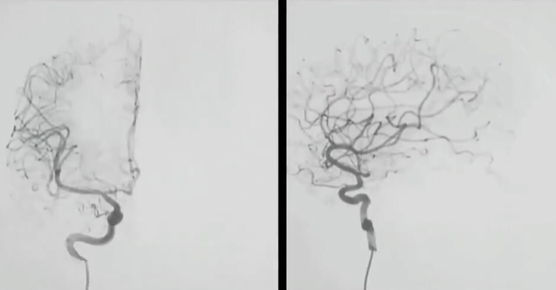
Postoperative DSA showed that the aneurysm was completely embolized,
no contrast agent filling was seen in the aneurysm cavity, and the parent artery was patent
Clinical Implications
1. The Illusion of Being "Alert": A transient disturbance of consciousness following an aneurysm rupture that resolves on its own can easily be mistaken for a "false alarm." In reality, a subarachnoid hemorrhage may have already occurred; seek immediate medical attention.
2. Headaches Are No Small Matter: A sudden "worst headache of your life," even if it subsides quickly, requires immediate medical evaluation.
3. Controlling Blood Pressure is Like Diffusing a Bomb: 70% of brain aneurysm ruptures are related to high blood pressure. Regular medication adherence and blood pressure control are far more effective than any health supplements.
The endpoint of aneurysm interventional treatment is not merely the completion of the procedure, but the patient's long-term favorable neurological functional outcome. We adhere to standardized postoperative antiplatelet management and imaging follow-up, and continuously study how to achieve a balance between dense embolization and perforator protection, as well as individualized considerations, for complex aneurysms like those in the M2 segment. "Old Wang's" new chapter continues, and the Neurological Medical Center's commitment to safeguarding cerebrovascular health never ceases.
Introduction to the Neuromedical Center
The Neurological Medical Center of Gansu Wuwei Cancer Hospital is a discipline integrating clinical care, teaching, scientific research, and talent cultivation. Its services span multiple fields including Neurology, Neurosurgery, Neurointervention, Neurocritical Care, and Neurorehabilitation. Patients can receive "one-stop" comprehensive diagnosis and treatment services at the center, ranging from disease diagnosis, treatment, rehabilitation, prevention, psychological care, and health education to long-term follow-up. The department has a well-structured team with strong technical expertise and extensive medical experience. It currently has 1 standing expert from the Neurosurgery Department of the First Hospital of Lanzhou University, 2 associate chief physicians, 3 attending physicians, 3 resident physicians (including 4 with master's degrees), and 11 nursing staff.
【Scope of Diagnosis and Treatment in the Neural Medical Center】
1. Neurology Specialty: Diagnosis and treatment of cerebrovascular diseases such as cerebral infarction and cerebral hemorrhage, peripheral neuropathies, spinal cord lesions, central nervous system demyelinating diseases, movement disorders (e.g., Parkinson's disease), neuromuscular junction disorders (e.g., myasthenia gravis), as well as headaches, vertigo, epilepsy, sleep disorders, and more.
2. Neurosurgery Specialty: Surgical treatment and care for common conditions including brain tumors, cerebral hemorrhage, cerebrovascular malformations, cerebral aneurysms, and traumatic brain injury. This encompasses microsurgery for brain tumors, transsphenoidal pituitary tumor surgery, surgery for severe traumatic brain injury, microvascular decompression for trigeminal neuralgia and hemifacial spasm, surgery for congenital cranial malformations, frameless stereotactic navigation-guided biopsy of intracranial tumors, carotid endarterectomy, deep brain stimulation (DBS) for Parkinson's disease, stereoelectroencephalography (SEEG) for epilepsy, and ventriculoperitoneal shunt for hydrocephalus.
3. Neurointervention Specialty: Intravenous and intra-arterial thrombolysis for stroke; cerebral angiography (via transradial or transfemoral approach); spinal cord angiography; mechanical thrombectomy for intracranial large vessel occlusion; angioplasty and stenting for intracranial arterial stenosis; carotid artery stenting; vertebral artery stenting; and endovascular coiling of cerebral aneurysms.
Our center maintains long-term collaboration with renowned specialized institutions such as Beijing Tiantan Hospital, Huashan Hospital affiliated with Fudan University, West China Hospital of Sichuan University, The First Hospital of Lanzhou University, and The Second Hospital of Lanzhou University, forming a medical consortium. We also regularly invite distinguished experts from within and outside the province for ward consultations and surgical guidance to better serve our patients.
Clinic Address:
Room 508, Outpatient Department, Central Campus, Gansu Wuwei Cancer Hospital
10th Floor, Inpatient Building, Central Campus, Gansu Wuwei Cancer Hospital


