
A Guide to Gynecological Tumors | Understanding Endometrial Cancer: A Comprehensive Overview
A Guide to Gynecological Tumors | Understanding Endometrial Cancer: A Comprehensive Overview
1. Introduction
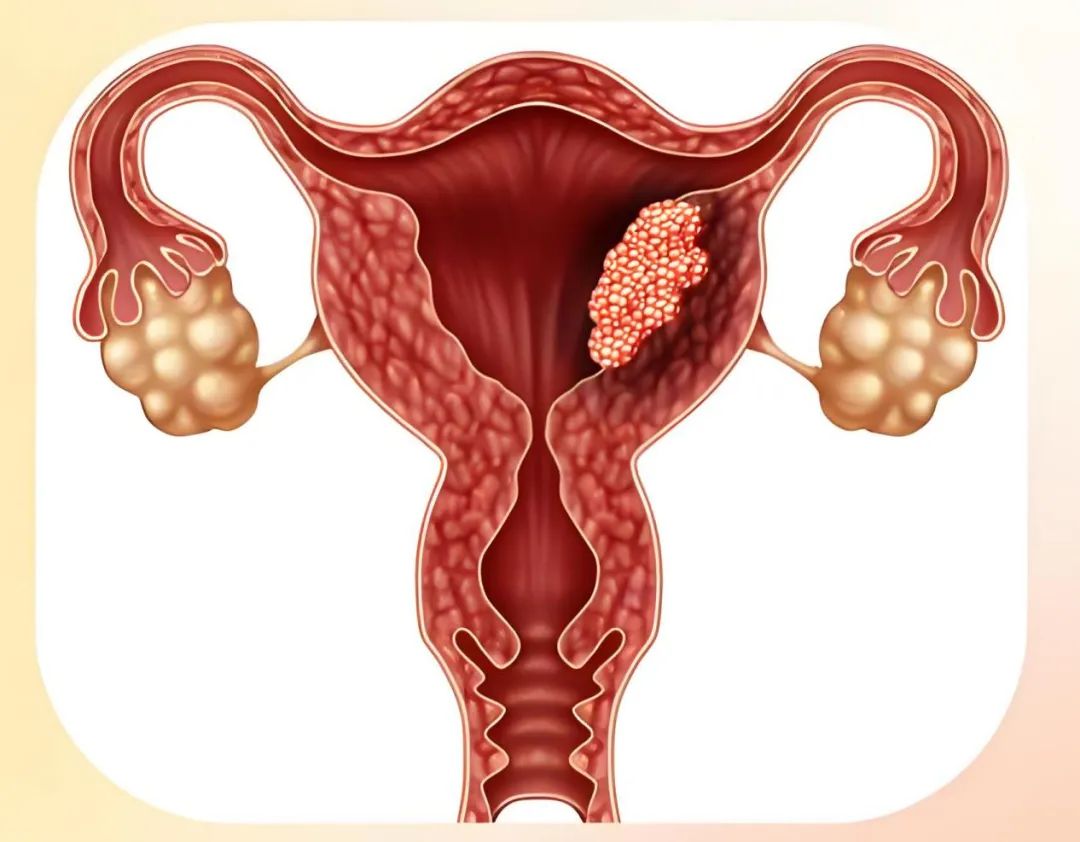
Endometrial cancer is a malignant tumor originating from the endometrial epithelium, accounting for 20%–30% of gynecologic malignancies and ranking as the second most common gynecologic malignancy. It is classified into two types:
Type I (estrogen-dependent, 70%–80%): Includes G1/G2 endometrioid adenocarcinoma, which is well-differentiated and has a favorable prognosis.
Type II (non-estrogen-dependent, 10%–20%): Includes G3 endometrioid adenocarcinoma and other non-endometrioid adenocarcinomas (such as serous carcinoma, clear cell carcinoma, carcinosarcoma, and undifferentiated/dedifferentiated carcinoma), which are highly aggressive with a poor prognosis.
2. Epidemiology
Incidence: In 2021, there were 417,367 new cases and 97,370 deaths globally. It ranks first in incidence in developed countries and some developed cities in China, accounting for about 7% of all female cancers and 20%–30% of malignant tumors of the reproductive tract. Age distribution: Predominantly affects postmenopausal women (aged 50–70), but the number of younger patients has increased in recent years (associated with obesity). Risk factors include obesity, diabetes, hypertension, anovulatory disorders (such as PCOS), nulliparity, late menopause, exogenous estrogen exposure (without progesterone antagonism), and Lynch syndrome.
3. Etiology
Estrogen excess and hormonal imbalance are key risk factors. Other high-risk factors include obesity, diabetes, prolonged infertility, early menarche, and late menopause.
4. Pathology
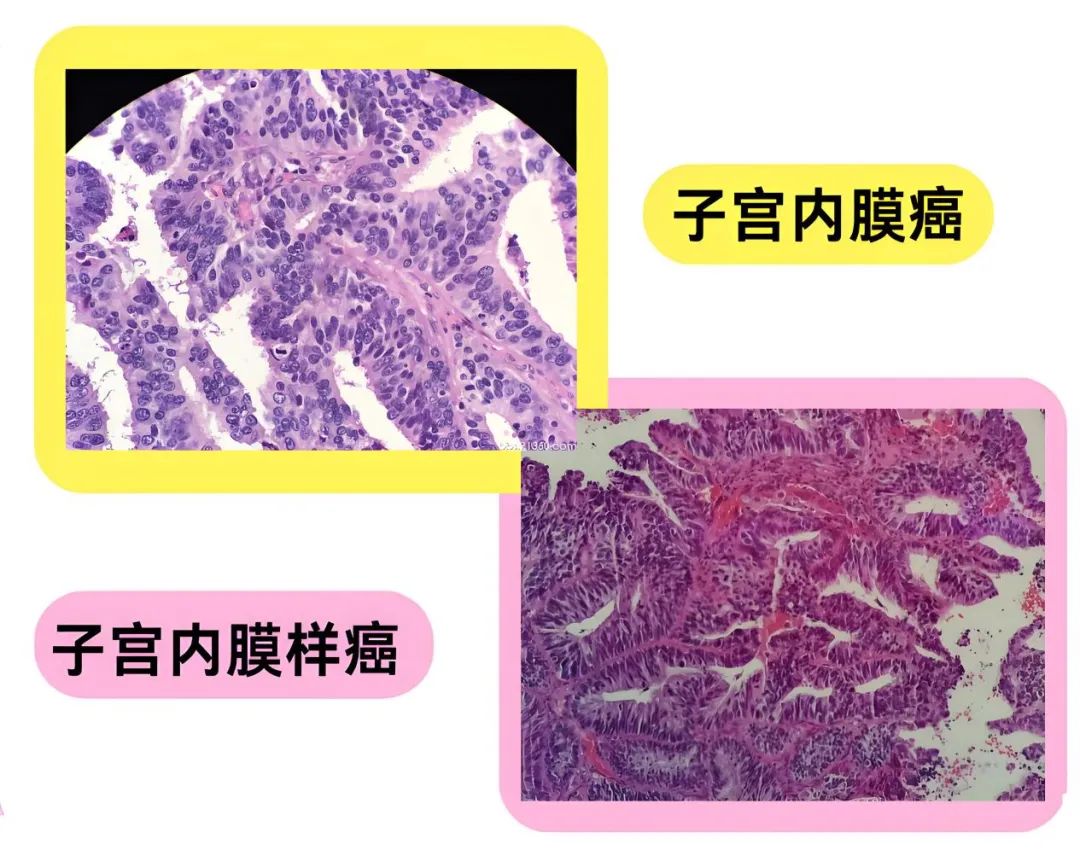
Precancerous lesions: Atypical hyperplasia of the endometrium/endometrial intraepithelial neoplasia.
Endometrioid carcinoma: Grading is based on architectural features (e.g., if ≥50% of the tumor shows marked nuclear atypia, the FIGO grade is increased by one level from the original classification).
FIGO Grade 1: Solid growth pattern <5%
FIGO Grade 2: Solid growth pattern 6–50%
FIGO Grade 3: Solid growth pattern ≥50%
Serous carcinoma: High cytological grade with marked nuclear pleomorphism, large nucleoli, and prominent mitotic activity. Tumor giant cells and psammoma bodies may sometimes be seen.
Clear cell carcinoma: Characterized by cells with abundant clear cytoplasm, exhibiting several architectural patterns: papillary, glandular, tubulocystic, and diffuse, which may form "hobnail" structures.
Undifferentiated carcinoma and dedifferentiated carcinoma: Undifferentiated carcinoma is a malignant epithelial tumor without obvious cell lineage differentiation.
Dedifferentiated carcinoma consists of undifferentiated carcinoma and differentiated components (usually FIGO Grade 1 or 2 endometrioid carcinoma).
Mixed carcinoma: Mostly a mixture of endometrioid and high-grade non-endometrioid components (usually serous).
Carcinosarcoma: Contains both malignant epithelial (carcinomatous) and malignant mesenchymal (sarcomatous) components. Uterine carcinosarcoma was originally classified as a sarcoma, but molecular biological evidence shows that the tumor cells exhibit epithelial-mesenchymal transition features. Therefore, in the latest WHO classification, carcinosarcoma is considered a type of endometrial carcinoma rather than a mixed tumor.
Other types of endometrial carcinoma: Mesonephric carcinoma, gastric-type adenocarcinoma, etc.
5. Clinical Manifestations
Approximately 90% of patients present with symptoms of vaginal bleeding or vaginal discharge.
1. Vaginal Bleeding: The early manifestation of endometrial cancer is primarily postmenopausal bleeding, usually in small amounts. In premenopausal women, it may present as increased menstrual flow, prolonged menstruation, or menstrual irregularities.
2. Vaginal Discharge: Typically bloody or serous in nature. If complicated by infection, the discharge may become purulent with blood and foul-smelling.
3. Lower Abdominal Pain and Other Symptoms: If the tumor involves the internal cervical os, it can lead to pyometra (intrauterine pus accumulation), causing lower abdominal distension, pain, and cramping. Tumor invasion into surrounding uterine tissues or compression of nerves may result in lower abdominal or lumbosacral pain. In advanced stages, symptoms such as anemia, weight loss, and cachexia may develop.
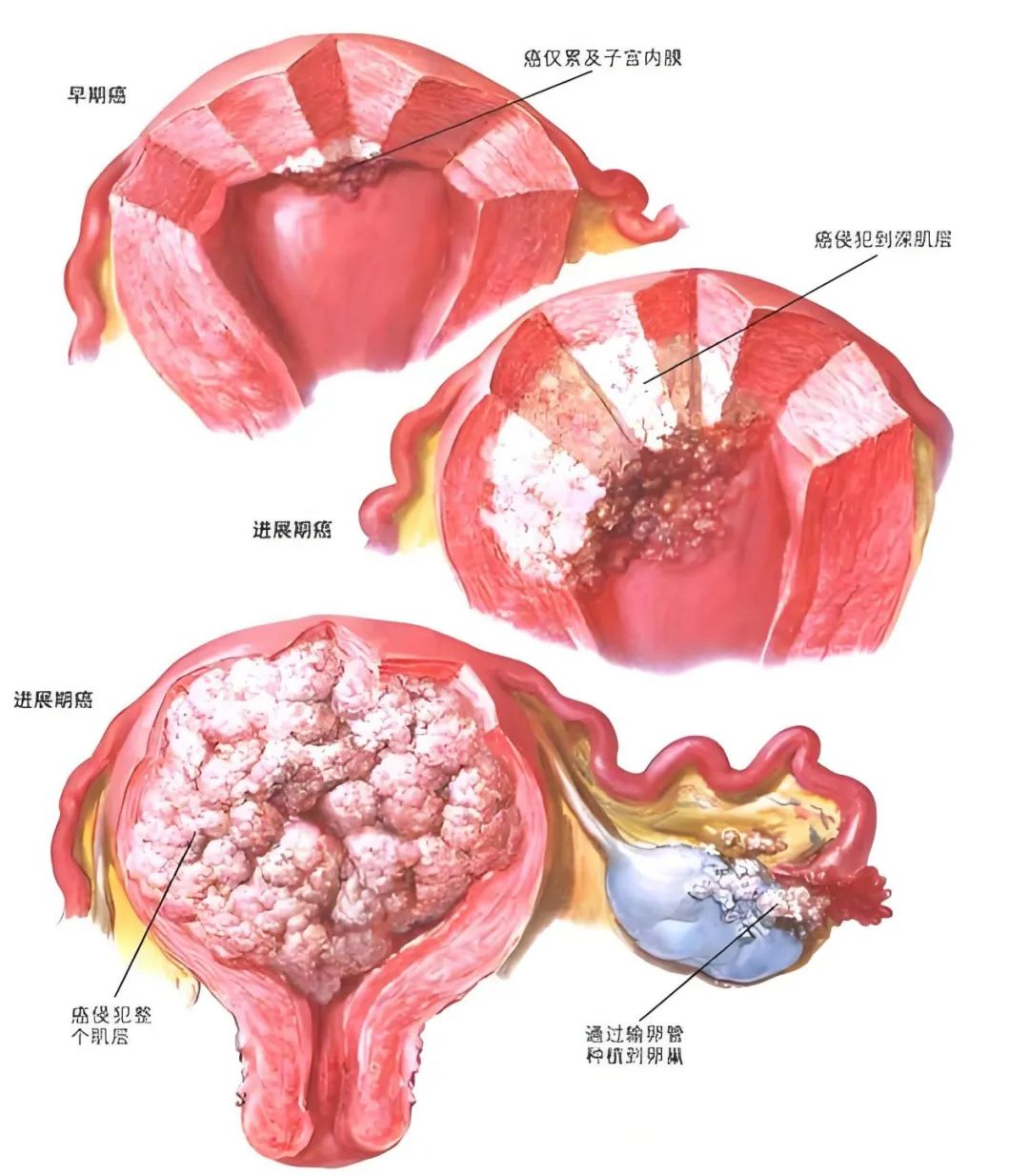
6. Tumor staging
Stage I: The tumor is confined to the uterine corpus and ovaries.
Stage II: The tumor invades the cervical stroma but shows no extrauterine spread or extensive lymphovascular space invasion (LVSI), or invasive histological types invade the myometrium.
Stage III: Any histological type with local and/or regional spread.
Stage IV: The tumor invades the bladder and/or rectal mucosa and/or has distant metastasis.
7. Treatment
1. Surgery
Surgery is the mainstay treatment for endometrial cancer. For early-stage patients, the goals of surgery include surgical-pathological staging to accurately assess disease extent and prognosis-related factors, removal of the affected uterus and any potential metastatic lesions, and determination of the need for postoperative adjuvant therapy.
2. Radiotherapy
Radiotherapy is one of the effective treatment methods for endometrial cancer. Radiotherapy alone is only suitable for elderly and frail patients or those with severe comorbidities who cannot tolerate or are contraindicated for surgery, as well as for stage III or higher cases unsuitable for surgery. It includes intracavitary and external beam irradiation; among these, carbon ion radiotherapy can be considered as a treatment option for inoperable patients.
3. Chemotherapy
As a systemic treatment, chemotherapy is indicated for advanced or recurrent endometrial cancer, or for postoperative patients with high-risk factors for recurrence, aiming to reduce extra-pelvic distant metastasis.
4. Hormonal Therapy
Primarily used for early-stage endometrial cancer patients who wish to preserve fertility; it can also serve as one of the comprehensive treatment options for advanced or recurrent endometrial cancer patients.
5. Traditional Chinese Medicine (TCM) Therapy
TCM therapy can be administered after surgery and chemoradiotherapy to strengthen the body, enhance the patient's immune function, and support overall recovery.
8. Prognosis
The 5-year survival rate is over 90% for Stage I, 70%-80% for Stage II, 40%-60% for Stage III, and less than 20% for Stage IV.
Poor prognostic factors include high tumor grade, deep myometrial invasion, lymph node metastasis, Type II histology (non-endometrioid carcinoma), and advanced age.
9. Follow-up
1. How often should follow-up be conducted after endometrial cancer treatment?
• Patients should have follow-up visits every 3-6 months in the first 2-3 years after completing treatment, and every 6-12 months thereafter.
2.What follow-up tests are required?
• Health education on possible recurrence symptoms, lifestyle modifications, obesity management, exercise, smoking cessation, nutritional counseling, sexual health, and the use of vaginal dilators and lubricants:
• CA125 should be rechecked during follow-up if it was elevated previously;
• Imaging studies such as CT, MRI, or PET-CT may be needed when necessary (e.g., when CA125 is elevated or suspicious positive lesions are detected by ultrasound).
Department Overview

Department of Radiation Oncology II (Gynecologic Oncology Radiotherapy)
As a specialized radiation therapy unit within the Gynecologic Oncology Group, our department is dedicated exclusively to the radiotherapy treatment of gynecologic malignancies. Equipped with state-of-the-art radiation therapy equipment and staffed by a highly skilled multidisciplinary team, we provide precise, standardized, and individualized comprehensive care for patients with gynecologic cancers.
●Professional Team
The department currently has a professional team of 14 members, including 1 chief physician, 1 attending physician, 4 resident physicians (5 of whom hold master's degrees), and 8 nurses - a dynamic and knowledgeable technical workforce. Department Director Zhao Fengju, Chief Physician, has over 30 years of experience in radiotherapy and is a rare expert in oncology in Northwest China. She serves as Chairperson of the Gansu Provincial Anti-Cancer Association's Brachytherapy Committee and Vice Chairperson of the Northwest Gynecologic Oncology and Brachytherapy Committee. She specializes in comprehensive treatment of gynecologic cancers including chemoradiotherapy and immunotargeted therapy, and has pioneered external beam radiotherapy techniques such as CIRT and IGRT for gynecologic cancers, as well as three-dimensional brachytherapy, interstitial implantation therapy, and painless brachytherapy, bringing extensive clinical experience in oncologic chemoradiotherapy. The department also receives technical and academic guidance from renowned experts including:
Professor Wang Junjie, Chairperson of the National Radiotherapy Committee, Director of the Radiation Oncology Department at Peking University Third Hospital, and President of the Lanzhou Heavy Ion Center
Professor Li Sha, Director of the Radiation Oncology Department at the Army Medical University General Hospital
Professor Du Lanning, from the First Hospital of Lanzhou University
●Treatment Scope
The department currently has a team of 14 medical staff, including 1 chief physician, 1 attending physician, and 4 resident physicians. The department primarily provides carbon ion radiotherapy, photon radiotherapy (including IMRT, VMAT, etc.), and brachytherapy for various common female malignancies such as cervical cancer, endometrial cancer, ovarian cancer, vulvar cancer, vaginal cancer, and breast cancer, as well as other malignant tumors including gastrointestinal cancers, urological cancers, and soft tissue sarcomas. Additionally, the department offers comprehensive treatment including chemotherapy, targeted therapy, immunotherapy, and cellular immunotherapy for various malignant tumors.

Lanzhou Heavy Ion Center Contact Information
Director Li: +86 166 0931 3666
Teacher Yan: +86 176 9325 0603

