
Which Head and Neck Cancers Are Suitable for Radiotherapy?
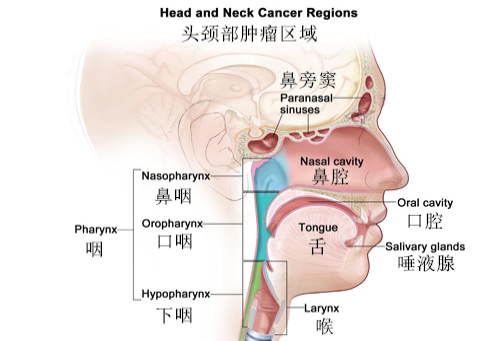
The head and neck region encompasses all organs above the neck, including the oral cavity, nasal cavity, paranasal sinuses, pharynx, larynx, thyroid, and salivary glands. Malignant tumors arising in these areas are collectively termed head and neck cancers. The primary treatments for head and neck cancers include surgery, radiotherapy, chemotherapy, and immunotherapy. But which head and neck cancers are best treated with radiotherapy?
Radiotherapy is one of the mainstays of treatment for head and neck cancers, with approximately 70% of patients requiring radiotherapy at some stage of their disease. It can be used as curative therapy or as adjuvant treatment before or after surgery.
Nasopharyngeal Cancer
Nasopharyngeal cancer (NPC) originates in the nasopharynx and is highly prevalent in China, ranking first among head and neck malignancies. NPC is endemic, with strong regional, racial, and familial clustering. Radiotherapy is highly sensitive to NPC and serves as the primary curative treatment. Early-stage NPC can often be cured with radiotherapy alone, while advanced cases require combined approaches (radiotherapy ± chemotherapy).
Recent advances in imaging and radiotherapy technologies—such as intensity-modulated radiotherapy (IMRT), volumetric-modulated arc therapy (VMAT), and proton/heavy ion therapy—have significantly improved local control rates, survival outcomes, and reduced complications. For locally advanced NPC, concurrent chemoradiotherapy is standard. For recurrent or metastatic NPC, palliative radiotherapy may be added to systemic therapies (chemotherapy, targeted therapy, immunotherapy).

Oral Cancer
Oral cancer arises from malignant lesions in the oral mucosa, accounting for 8.2% of all malignancies. Common subtypes include tongue cancer, gingival cancer, buccal cancer, and floor-of-mouth cancer, with tongue cancer comprising 40–60% of cases. Risk factors include smoking, alcohol use, betel nut chewing, poor oral hygiene, and chronic irritation.
Surgery and radiotherapy are primary treatments. Early-stage oral cancer is typically managed surgically, with adjuvant radiotherapy based on pathology. For locally advanced cases, neoadjuvant chemotherapy + surgery + postoperative chemoradiotherapy or definitive chemoradiotherapy is recommended. For inoperable patients, radical radiotherapy or chemoradiotherapy achieves outcomes comparable to surgery. Palliative radiotherapy is used for recurrent/metastatic disease.

Oropharyngeal Cancer
Oropharyngeal cancer includes malignancies of the base of tongue, tonsils, soft palate, and pharyngeal walls. HPV infection, smoking, and alcohol are major risk factors. Squamous cell carcinoma (SCC) is the most common histology.
Radiotherapy plays a pivotal role. Early-stage (T1-2N0) oropharyngeal cancer can be treated with surgery or radiotherapy alone. For locally advanced cases, concurrent chemoradiotherapy is standard. HPV-positive tumors show higher radiosensitivity and better prognosis. Palliative radiotherapy is an option for recurrent/metastatic disease.

Hypopharyngeal Cancer
Hypopharyngeal cancer involves the pyriform sinus, posterior pharyngeal wall, or postcricoid area. Smoking and alcohol are key risk factors. SCC is the predominant histology. Due to its hidden anatomy and late-stage diagnosis, prognosis remains poor.
Treatment mirrors other head and neck cancers: surgery ± adjuvant radiotherapy for early stages, and chemoradiotherapy or definitive chemoradiotherapy for advanced cases. Palliative radiotherapy is used for inoperable or metastatic disease.
Laryngeal Cancer
Laryngeal cancer includes supraglottic, glottic, and subglottic tumors. Smoking and alcohol are major risk factors. Symptoms include hoarseness, pain, and hemoptysis.
For early-stage (T1-2N0) glottic cancer, radiotherapy or surgery achieves similar outcomes. For supraglottic/subglottic cancer, surgery is preferred, with adjuvant radiotherapy based on pathology. Definitive chemoradiotherapy may preserve laryngeal function in select cases. Palliative radiotherapy is used for advanced/metastatic disease.
Nasal and Paranasal Sinus Cancer
These cancers arise in the nasal cavity or paranasal sinuses (maxillary, ethmoid, frontal, sphenoid). Risk factors include chronic inflammation and carcinogen exposure. SCC is the most common subtype.
Early-stage cases are treated surgically, with adjuvant radiotherapy as needed. For advanced disease, neoadjuvant chemotherapy + surgery + postoperative chemoradiotherapy or definitive chemoradiotherapy is recommended. Palliative radiotherapy is used for inoperable or metastatic cases.
Thyroid Cancer
Thyroid cancer includes papillary, follicular, medullary, and anaplastic subtypes. Radiotherapy is not routinely used but plays a role in specific scenarios:
· Postoperative iodine-131 therapy for high-risk papillary/follicular cancers to ablate residual tissue.
· External beam radiotherapy for locally advanced/unresectable tumors.
· Chemoradiotherapy for anaplastic thyroid cancer.

Salivary Gland Cancer
Salivary gland cancer is a malignant tumor originating in salivary gland tissues, including parotid gland cancer, submandibular gland cancer, and sublingual gland cancer. Its development is associated with factors such as chronic inflammatory stimulation and radiation injury. Salivary gland cancer encompasses diverse histopathological types, including acinic cell carcinoma, mucoepidermoid carcinoma, adenoid cystic carcinoma, and malignant mixed tumors. Due to its atypical early symptoms, it is often missed or misdiagnosed, with most patients presenting at advanced stages.
Surgery is the primary treatment for salivary gland cancer. Early-stage cases can achieve favorable outcomes with surgery alone. For locally advanced cases, comprehensive treatment centered on surgery is recommended, with adjuvant radiotherapy administered postoperatively based on pathological findings. For recurrent or metastatic disease, palliative radiotherapy may be integrated into systemic therapies (chemotherapy, targeted therapy, immunotherapy) to manage symptoms and improve quality of life.
The head and neck region houses critical organs for vision, hearing, speech, breathing, and swallowing. Surgical resection is often challenging due to anatomical complexity. Radiotherapy offers precise tumor targeting while sparing healthy tissues. Advanced techniques like IMRT, VMAT, SBRT, and proton/heavy ion therapy enable personalized treatment plans.

Common Radiotherapy Techniques
Three-dimensional conformal radiotherapy (3D-CRT), intensity-modulated radiotherapy (IMRT), volumetric-modulated arc therapy (VMAT), and stereotactic radiosurgery (SBRT) are widely used in clinical practice. Additionally, brachytherapy (internal radiation), spatial fractionation radiotherapy (SFRT), image-guided radiotherapy (IGRT), and the rapidly evolving proton therapy and carbon ion radiotherapy (CIRT) play pivotal roles in modern radiotherapy.

Department Profile
Gansu Wuwei Cancer Hospital Radiation Oncology Department V specializes in treating head/neck cancers, central nervous system tumors, and lymphomas. Services include neoadjuvant, concurrent, and adjuvant radiotherapy (including heavy ion therapy), immunotherapy, and targeted therapy.
Expert Team
Led by Dr. Hu Tingchao, the team collaborates with international experts (e.g., Germany’s Prof. Haofei, Japan’s Prof. Tsumura) and utilizes cutting-edge radiotherapy technologies. Dr. Hu has 20 years of experience in head/neck and brain tumor radiotherapy, including heavy ion therapy and stereotactic radiosurgery (SBRT).

Department Director Profile

Hu Tingchao,Director, Department V of Radiation Oncology,Gansu Wuwei Cancer Hospital(Specializing in
Head and Neck Tumor Radiotherapy)
Dr. Hu Tingchao has 20 years of clinical, teaching, and research experience in tumor radiotherapy. His primary expertise lies in carbon ion radiotherapy (CIRT), chemotherapy, targeted therapy, and immunotherapy for head/neck and intracranial tumors. He is particularly skilled in:
• Comprehensive postoperative management of gliomas.
• Treatment of recurrent/metastatic head and neck cancers.
• Stereotactic radiosurgery (SBRT) for brain metastases with hippocampal protection during prophylactic cranial irradiation.
• Stereotactic radiotherapy for benign and malignant intracranial tumors.

