
A New Treatment Option for Tracheal Adenoid Cystic Carcinoma: Heavy Ion (Carbon Ion) Therapy
A New Treatment Option for Tracheal Adenoid Cystic Carcinoma: Heavy Ion (Carbon Ion) Therapy
March 2026 – Professor Zhang Yanshan reported that over the past eight years, the Wuwei Heavy Ion Center has treated a total of 124 patients with adenoid cystic carcinoma (ACC). The number of treated cases, follow-up data, and long-term outcomes have all reached internationally advanced levels, establishing the center as one of the key institutions for heavy ion (carbon ion) therapy for adenoid cystic carcinoma both in China and globally. These 124 ACC cases involved various anatomical sites, including ACC of the head and neck, ACC of the lung, and ACC of the pelvic cavity and vagina. Herein, we summarize and report on 12 cases of tracheal adenoid cystic carcinoma.
Tracheal adenoid cystic carcinoma is often referred to as the "hidden killer in the airway" due to its tendency to infiltrate along nerve bundles, high local recurrence rate, and insensitivity to conventional radiotherapy. In Wuwei, Gansu Province, a cutting-edge technology hailed as a "pillar of the nation" – heavy ion (carbon ion) therapy – is opening a new lifeline for patients with tracheal adenoid cystic carcinoma, supported by robust clinical data. The Wuwei Heavy Ion Center is equipped with China's first heavy ion treatment system boasting complete independent intellectual property rights. Since the treatment of the first patient in November 2018, the center has completed an eight-year journey. As of March 2026, more than 2,800 patients have been treated cumulatively for over 100 disease types, including 12 cases of tracheal adenoid cystic carcinoma. Here, we introduce and summarize our treatment experience with this relatively rare disease, aiming to help more patients make better-informed choices.
I. Advantages and Disadvantages of Surgery
For the treatment of tracheal adenoid cystic carcinoma (TACC), before the availability of heavy ion therapy as a highly effective and low-toxicity local treatment modality, surgery was the only curative treatment option. The advantages of surgery are: early-stage patients can achieve cure, with ideal long-term survival rates after complete resection (R0); the resected specimen allows for definitive pathological diagnosis; intact tumor tissue can be obtained for pathological analysis and molecular biology testing; direct tumor resection provides rapid relief of symptoms such as dyspnea. The disadvantages of surgery are: due to the limited length of the trachea, the resectable length is restricted, resulting in a low rate of complete resection, with only 42–57% achieving R0 resection and a positive margin rate as high as 59–63%; surgical risks are considerable, with a mortality rate of approximately 1–25%; complications may include recurrent laryngeal nerve paralysis, anastomotic stenosis, and tracheoesophageal fistula; the extent of resection is limited: due to the limited length of the trachea, extensive resection makes anastomosis difficult. Surgery easily leads to metastasis and dissemination and cannot prevent long-term recurrence: there remains local recurrence (approximately 3.8%) and distant metastasis (approximately 24.9%). Most patients require combined radiotherapy: adjuvant radiotherapy is often needed postoperatively to compensate for the shortcomings of surgery.
II. Heavy ion therapy represents a new safe and effective treatment option for tracheal adenoid cystic carcinoma
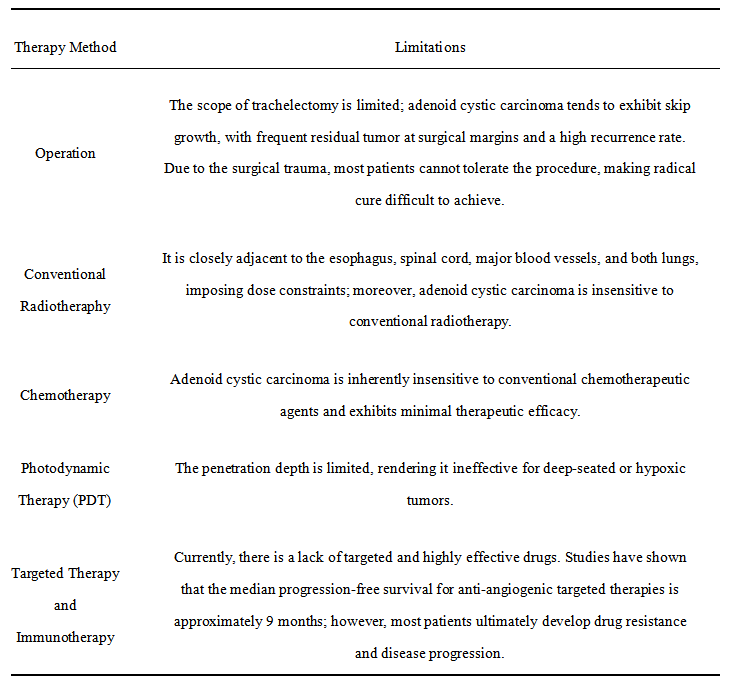
Tracheal adenoid cystic carcinoma generally occurs in the middle and lower segments of the trachea, adjacent to major blood vessels, the esophagus, and the spinal cord, making complete surgical resection difficult. The tumor is rich in stroma and myxoid material, with many hypoxic regions, rendering it highly resistant to conventional radiotherapy and chemotherapy. Due to its perineural invasion characteristics, it tends to spread along the tracheal wall and nerve bundles. Within the limited resection margin of the trachea, it is often impossible to completely prevent such spread, and distant metastasis (especially to the lungs) is common.
Heavy ion (carbon ion) therapy overcomes the limitations of the above treatments. The Bragg peak of heavy ions enables "precision blast" effects, releasing the majority of energy at the end of its range, precisely covering the primary tracheal lesion while protecting the spinal cord, esophagus, and major blood vessels. The relative biological effectiveness (RBE) of heavy ions is 2–5 times that of conventional photons, directly inducing double-strand breaks in tumor cell DNA, and is equally effective against hypoxic and radioresistant cells. Heavy ion therapy can cover the tumor itself, its invasion pathways, and regional lymph nodes, achieving "regional dissection" and effectively reducing the risk of local recurrence. Furthermore, heavy ions enable wide coverage, preventing spread along neural pathways.
III. Four core advantages of heavy ion therapy for tracheal adenoid cystic carcinoma:
- Rapid onset, quickly relieving dyspnea: For obstructions caused by the tumor, heavy ion therapy often achieves tumor regression early in the treatment course.
- Non-invasive, no risk of bleeding: Tracheal tumors carry a risk of massive bleeding even during bronchoscopic biopsy. However, heavy ion therapy is a non-invasive irradiation modality, completely avoiding procedure-related risks of bleeding and asphyxia.
- Adenoid cystic carcinoma is resistant to conventional radiotherapy, but the high relative biological effectiveness (RBE) of heavy ions can directly break the double-strand DNA of tumor cells, producing irreparable damage.
- Well tolerated even by elderly and frail patients: Age is not a contraindication for treatment; patients are eligible as long as their general medical condition is stable.
- The heavy ion radiation field can fully cover the primary tumor, its potential submucosal infiltration range, and regional lymph nodes, achieving "regional dissection." Heavy ions enable wide coverage, extensively encompassing the nerves within the tumor's range to prevent perineural spread. This is one of the advantages of heavy ion therapy for adenoid cystic carcinoma.
IV. Which patients with cystic adenocarcinoma of the trachea are eligible for heavy ion therapy?
✅ Priority Recommendations:
✅ Early-stage tracheal adenoid cystic carcinoma: heavy ion therapy can achieve non-invasive cure.
✅ Locally advanced cases, patients who are inoperable or unwilling to undergo surgery: heavy ion therapy can effectively inactivate the tumor.
✅ Oligometastatic (e.g., single or a few metastatic lesions in the lungs, bones, or other sites) stage IV patients.
✅ Postoperative recurrence or residual disease where repeat surgery is not feasible.
✅ Postoperative prophylactic irradiation.
⚠️ Use with Caution (limited efficacy):
⚠️ Diffuse, widespread metastases involving multiple organs such as the lungs, liver, and bones.
V. Case Sharing
Patient Mr. Wang, male, 70 years old, diagnosed with adenoid cystic carcinoma of the middle and lower trachea.
In March 2024, the patient developed cough, sputum production, blood-streaked sputum, and hoarseness. Chest CT showed localized thickening of the left wall of the trachea. PET-CT indicated thickening of the left wall of the lower main bronchus with increased metabolic activity. Electronic bronchoscopy with biopsy confirmed adenoid cystic carcinoma. Without knowledge of heavy ion therapy, the patient underwent multiple sessions of bronchoscopic photodynamic therapy at another hospital on December 16, 17, and 18, 2024. After treatment, cough and sputum production improved somewhat. In September 2025, the patient experienced worsening irritative cough, increased airway secretions, and difficulty expectorating. The original hospital arranged for another session of bronchoscopic photodynamic ablation. However, the patient learned about heavy ion therapy and came to the Wuwei Heavy Ion Center to consult Professor Zhang Yanshan. CT examination revealed irregular thickening of the left tracheal wall with a local protrusion extending into the lumen. In October 2025, the patient received carbon ion therapy at the Wuwei Heavy Ion Center. During the course of heavy ion therapy, the patient's symptoms of cough, sputum production, and blood-streaked sputum improved significantly. Six months after treatment, the patient's symptoms had completely resolved. He now coughs only when exposed to irritating odors; all other symptoms have completely resolved.
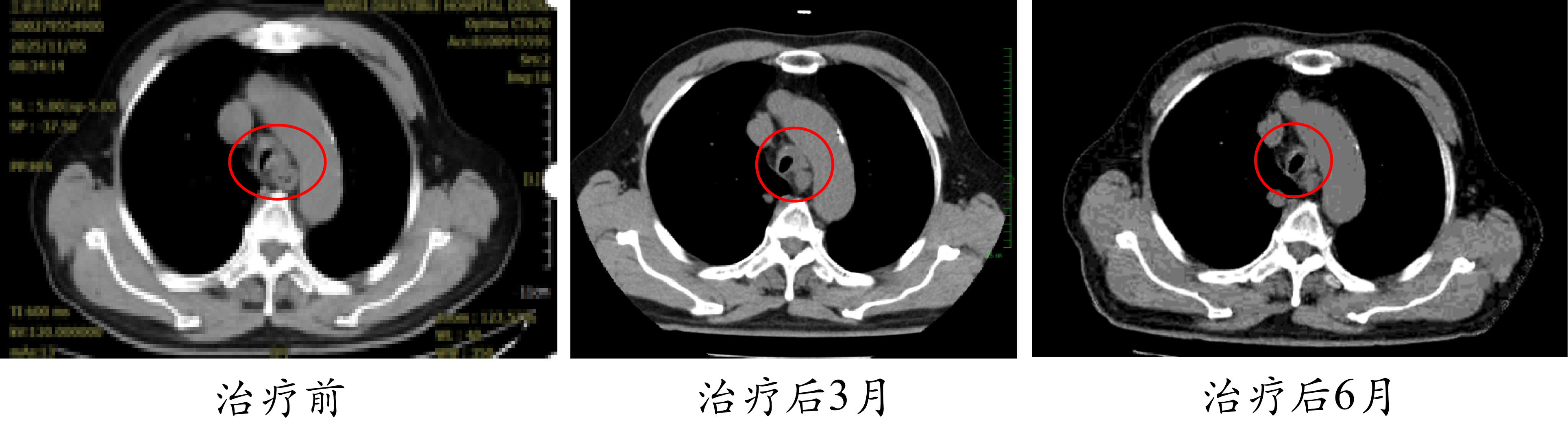
This case confirms the unique value of heavy ion therapy for tracheal adenoid cystic carcinoma that is locally recurrent and resistant to conventional treatment modalities. It is non-invasive, has no or only very mild side effects, and can be easily tolerated by very elderly patients. The treatment significantly improved the patient's quality of life and achieved excellent local control.
Case provided by: Dr. Yang Yuling
Department: Radiation Oncology Center Ⅰ(International Medical Department Ⅰ)
VI. Conclusion:
Due to its anatomical location, growth characteristics, treatment response, and recurrence patterns, tracheal adenoid cystic carcinoma often cannot be completely resected by surgery. Conventional radiotherapy has very poor efficacy, while chemotherapy and targeted therapy also offer limited benefits in improving survival. At the Wuwei Heavy Ion Center, we have demonstrated with real-world data that heavy ion therapy—characterized by high efficacy, low toxicity, and precision—is emerging as a new treatment option for tracheal adenoid cystic carcinoma. Regardless of whether the disease is early or advanced, or regardless of the patient's comorbidities, heavy ion therapy offers advantages that surpass surgery across the board. The response rate of heavy ion therapy for tracheal adenoid cystic carcinoma is 100%.
VII. General Information of Adenoid Cystic Carcinoma of the Trachea
Extremely low incidence: The incidence of primary tracheal malignant tumors is 0.1–0.26 per 100,000 population. Tracheal adenoid cystic carcinoma accounts for 10–20% of all primary tracheal malignant tumors, making it the second most common primary tracheal malignant tumor after squamous cell carcinoma. Age and gender at onset: The average age at diagnosis is approximately 48–51 years, with a slight female predominance (male-to-female ratio approximately 1:1.17 to 1:1.38). Slow growth and insidious course: The average interval from symptom onset to diagnosis is 12.5 months. It is easily misdiagnosed as asthma, COPD, or pneumonia. Common symptoms (in order of incidence): Dyspnea (approximately 86%), cough (approximately 58%), shortness of breath (approximately 37%), hemoptysis (approximately 15%). Predominant location: The distal trachea/near the carina is more common. Most commonly used diagnostic tests: CT + bronchoscopy (accounting for approximately 72%), which can determine tumor location, extent, regional invasion, and pulmonary metastases, and can confirm the diagnosis through biopsy pathology. Pathological and invasive characteristics: Tracheal adenoid cystic carcinoma originates from the minor salivary glands in the submucosa of the trachea. It tends to spread submucosally and perineurally, leading to a high rate of positive surgical margins. Lymph node metastasis: Approximately 8–22%. Distant metastasis: Approximately 18–25%, most commonly to the lungs (approximately 44%). Treatment: In the past, treatment relied primarily on surgery. Surgery was previously the first-line treatment, but complete resection (R0) was achieved in only approximately 42–57%. Postoperative radiotherapy was often used for patients with positive margins or incomplete resection. Now, with heavy ion therapy, adenoid cystic carcinoma at all stages can be addressed. As a local treatment modality, heavy ion therapy is effective, safe, and reliable, with a response rate reaching 100%. However, heavy ion therapy cannot treat systemic metastatic adenoid cystic carcinoma. Chemotherapy does not significantly improve survival in adenoid cystic carcinoma. As of June 2026, no clearly effective novel drugs have been identified for tracheal adenoid cystic carcinoma, and some carry the risk of inducing rapid disease progression. Current research is focused on the following directions: First, NOTCH signaling pathway inhibitors are the most clearly defined targeted direction at present. Approximately one-quarter of adenoid cystic carcinoma patients harbor NOTCH gene mutations, and such patients typically have a worse prognosis. Drugs targeting this pathway, such as AL101, have achieved disease control in nearly 70% of patients in clinical trials, with some patients experiencing tumor shrinkage. However, a major issue with this class of drugs is that when used as monotherapy, the tumor often progresses again within a few months. Second, multi-target anti-angiogenic agents. Representative drugs include regorafenib and the domestic drugs anlotinib and apatinib. Their main effect is to stabilize the disease and delay tumor progression, but they rarely cause significant tumor shrinkage when used alone. Researchers are exploring combinations of these drugs with immunotherapy or other targeted agents. Third, targeted therapy against the MYB protein. The MYB protein is the most core driver of adenoid cystic carcinoma pathogenesis and is aberrantly expressed in more than half of patients. However, due to the unique structure of this protein, no drug can directly and effectively target it yet. Although researchers have attempted indirect inhibition by targeting its upstream signals, clinical trials have not yet achieved breakthrough efficacy. This remains a highly promising but currently unresolved challenge. Finally, in terms of immunotherapy, conventional PD-1 inhibitor monotherapy is ineffective because this type of tumor is a "cold tumor" that cleverly evades attack by the immune system. Scientists have discovered that a novel class of drugs called "STING agonists" may reverse this immunosuppressive state. There is a very rare case report of a patient whose tumor shrank significantly by 70% after receiving such combination therapy, but overall, this remains in very early stages of exploration.
Introduction to Wuwei Heavy Ion Center
The Wuwei Heavy Ion Center is a clinical application base for China's first heavy ion (carbon ion) treatment system with complete independent intellectual property rights. It receives technical support from the Institute of Modern Physics, Chinese Academy of Sciences, while clinical operations are managed by Gansu Wuwei Tumor Hospital. The center officially began cancer treatment in November 2018 and has cumulatively treated over 2,800 patients, expanding to more than 100 disease types, including lung cancer, pancreatic cancer, liver cancer, glioma, nasopharyngeal carcinoma, rectal cancer, various sarcomas, and others. As the only medical institution in the world operating two heavy ion (carbon ion) treatment systems simultaneously, Wuwei Tumor Hospital has achieved nine "global firsts" in technological innovation: pioneering precise treatment techniques under ventilator control; bladder cancer treatment under precise bladder volume control; single-session treatment using surgically implanted spacers between organs and tumors; developing China's first 360° rotating and elevating ion radiotherapy chair; globally completing the first cases of heavy ion (carbon ion) therapy for cardiac tumors; and pioneering dual Bragg peak lattice heavy ion (carbon ion) radiotherapy technology, among others. Leveraging 30 research platforms, including the CAS Key Laboratory of Heavy Ion Radiation Biology and the University of Sydney Biomedical Data Analysis and Visualization Laboratory, the center has conducted over 30 clinical studies on major disease types. To date, the center has published nine monographs, including the "Standard Operating Procedures for Carbon Ion Radiotherapy," establishing a comprehensive knowledge system covering physics technology, clinical diagnosis and treatment, and health management.
Author: Yang Yuling (Department 1, Radiotherapy Center)
Data Support: Chen Xuelian, Li Pengqing (Tumor Registry and Follow-up Office)
Reviewer: Zhang Yanshan (Vice President)
Date: June 1, 2026

