
Is Pelvic Fluid a Disease?
Is Pelvic Fluid a Disease?
Why Do Healthy People Have Fluid in the Pelvic Cavity?
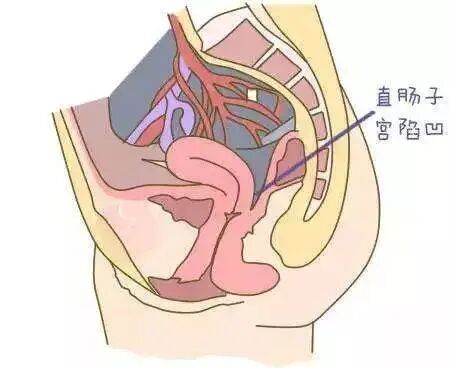
The pelvic and abdominal cavities of the human body are not dry. The peritoneum, omentum, intestines, and other tissues in these cavities secrete a certain amount of fluid, which typically serves to lubricate and protect the organs and tissues. These fluids are continuously secreted and simultaneously absorbed by the body. When standing, the pelvic cavity is positioned relatively low in the body, causing the secreted fluid to accumulate at the lowest point of the pelvis, specifically in the pouch of Douglas (the area between the uterus and rectum). At this point, an ultrasound can detect a certain depth of anechoic fluid in this recess, which is referred to as "pelvic effusion."
First and foremost, it is important to clarify that pelvic effusion is not a disease but rather a clinical manifestation. More precisely, it is a term used in ultrasound imaging to describe fluid in the pelvic cavity, which can be categorized into normal pelvic effusion (physiological pelvic effusion) and pathological pelvic effusion. Pelvic effusion in healthy individuals is physiological, with a typical volume of around 200ml.
What are the causes of physiological pelvic effusion?
Present in Everyone: The peritoneum secretes a small amount of serous fluid to protect organ surfaces and reduce friction between organs.
During Menstruation: Menstrual blood may flow backward through the fallopian tubes into the pelvic cavity. Ultrasound examination is generally not performed during this period.
During Ovulation: Around 14 days before the next menstrual cycle, bleeding from the ovulation site and follicular fluid released with the egg accumulate in the pelvic cavity. The effusion is usually within 2 cm in depth.
During the Luteal Phase: From ovulation to the day before the next menstruation, the rupture of the ovarian corpus luteum may cause slight bleeding, leading to fluid accumulation in the pelvis and abdominal pain. If the pain is mild and does not affect daily life, the effusion is often temporary and may resolve within 1–2 days, requiring no concern. However, if the pain is severe or the effusion persists, prompt medical attention is recommended.

Pelvic effusion can be detected through ultrasound examination. If the effusion depth is less than 3cm and no other discomfort symptoms are present, it generally requires no treatment. Even if the effusion depth slightly exceeds 3cm, considering the patient's medical history, menstrual cycle, ovulation period, luteal phase, and accompanying symptoms (such as the degree of abdominal pain), and after ruling out the possibility of pathological pelvic effusion, treatment may still be unnecessary.
How does pathological pelvic effusion occur?
Pathological pelvic effusion is typically accompanied by symptoms and is commonly observed in the following scenarios:
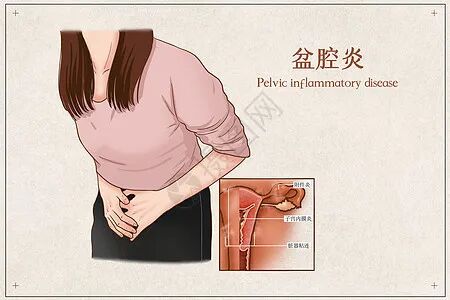
1. Pelvic Inflammatory Disease
When the peritoneum is exposed to inflammatory substances, foreign bodies, or other irritants, it can produce a large amount of exudative fluid. Patients may experience symptoms such as fever, lower abdominal pain, and abnormal vaginal discharge. Without these symptoms, the disease cannot be diagnosed. Gynecological examinations may reveal cervical motion tenderness, uterine or adnexal tenderness, and abnormal vaginal secretions. Pelvic effusion can be detected via color Doppler ultrasound, and abnormal white blood cell counts may be found in blood tests.
2. Ruptured Ectopic Pregnancy or Abortion Hemorrhage
Ectopic pregnancy, also known as tubal pregnancy, occurs when the embryo implants outside the uterine cavity, most commonly in the fallopian tube ampulla. Rupture can lead to hemorrhage. Typically, acute bleeding is critical and can cause life-threatening intra-abdominal hemorrhage within a short period. Patients often present with a history of missed periods, nausea, vomiting, vaginal bleeding, and lower abdominal pain.
3. Corpus Luteum Rupture
Rupture of the ovarian corpus luteum leads to bleeding from the site of rupture, with blood accumulating in the pelvic cavity. Patients may experience lower abdominal pain during the luteal phase that is difficult to relieve, often occurring after sexual intercourse or physical activity. Color Doppler ultrasound may reveal an adnexal mass with heterogeneous internal echoes, a significant amount of pelvic effusion (typically appearing as turbid fluid, often representing hemoperitoneum).
4. Ascites
Conditions such as tumors or cirrhosis can lead to massive ascites, often accompanied by pelvic masses. In such cases, the diagnosis is typically "massive ascites" rather than "pelvic effusion."
5. Pelvic and Abdominal Tuberculosis
This condition typically presents with symptoms such as low-grade fever, fatigue, weight loss, and infertility. Color Doppler ultrasound may reveal pelvic effusion, and tuberculosis tests return positive results.
Does pelvic inflammatory disease always cause pelvic effusion?

Pelvic inflammatory disease (PID) refers to a group of infectious conditions affecting the upper reproductive tract, including endometritis, salpingitis, tubo-ovarian abscess, and pelvic peritonitis. Based on the progression and severity, it is categorized into acute and chronic types.
In acute PID, congestion and edema of the affected area lead to the accumulation of significant inflammatory exudate, potentially forming abscesses. In chronic PID, adhesions around the lesion site hinder the flow and absorption of localized exudate, both of which can result in pelvic effusion. However, during the early stages of inflammation, when tissue degeneration and edema are mild, and inflammatory exudate has not yet formed or is minimal, ultrasound may not detect pelvic effusion even if gynecological examination reveals tenderness in the uterine or adnexal regions. Therefore, while PID may cause pelvic effusion, the presence of pelvic effusion on ultrasound does not necessarily indicate PID. Diagnosis of PID requires comprehensive analysis of medical history, gynecological examination, pathogen testing, and necessary auxiliary examinations. Before a definitive diagnosis is made by a doctor, the indiscriminate use of antibiotics should be avoided. In summary, the clinical manifestations of PID during the acute phase can vary significantly—ranging from obvious symptoms to complete absence of symptoms—and require professional differentiation and diagnosis by a physician.
How to treat pelvic effusion?
Physiological Pelvic Effusion: Typically asymptomatic or with mild symptoms. If ultrasound shows an effusion depth of less than 3cm, no treatment is usually required. Even if the depth slightly exceeds 3cm, intervention may still be unnecessary if the physician rules out pathological causes after considering medical history, menstrual cycle, ovulation period, and accompanying symptoms.
Pathological Pelvic Effusion: The underlying cause must be identified and treated accordingly. Conditions such as ectopic pregnancy or pelvic/abdominal tumors may require prompt surgical intervention. Therefore, initiating treatment without a clear diagnosis could delay proper management and potentially lead to severe or life-threatening consequences.
Treatment of Pelvic Effusion Caused by Acute Pelvic Inflammatory Disease
Supportive care: Bed rest with a semi-recumbent position helps confine inflammation by allowing pus to accumulate in the rectouterine pouch. Physical cooling, nutritional support, fluid replacement, and correction of electrolyte imbalances and acid-base disturbances are provided.
Antibiotic therapy: During acute episodes of pelvic inflammatory disease, doctors will prescribe targeted antibiotics based on the patient's vaginal secretion culture results. Hospitalization may be necessary if required. Self-administering oral antibiotics without guidance should be avoided to prevent antibiotic resistance and complications in subsequent treatments.
Surgical treatment: If there is no significant improvement after antibiotic therapy, hospitalization and timely re-examination are required, with surgery performed if necessary. Surgical approaches include abscess incision and drainage (which can be performed abdominally, vaginally, or laparoscopically), unilateral adnexectomy (suitable for women with unilateral tubo-ovarian abscess who wish to preserve fertility), and total hysterectomy with bilateral salpingo-oophorectomy (for severe cases, older patients, or those without fertility desires).
Sexual Partner treatment: For patients with acute pelvic inflammatory disease, any sexual partners from within 60 days prior to symptom onset should undergo pathogen testing and treatment.
Symptomatic treatment: Modalities such as local heat therapy use warm, benign stimulation to promote pelvic blood circulation, improve tissue nutrition, and enhance metabolism, thereby facilitating inflammation resolution. Laser therapy can reduce inflammation, relieve pain, and promote tissue repair. Magnetic wave therapy, with its high microwave absorption rate, shallow penetration, and even heat distribution, can precisely target the treatment area.
Note: Physiotherapy is contraindicated for patients who are menstruating or pregnant, have gynecological malignancies, vaginal bleeding, or underlying medical conditions such as cardiac, hepatic, or renal insufficiency, active tuberculosis, high fever, or allergic constitutions.
How to care for your health if you have pelvic effusion?
1. Patients with significant abdominal pain should rest adequately and may take oral non-steroidal anti-inflammatory drugs, such as ibuprofen. If the pain does not improve within 48-72 hours after medication, consult a doctor.
2. Engage in moderate exercise to enhance physical fitness.
3. Avoid sexual activity during the treatment of pelvic inflammatory disease. The specific duration of avoidance should be discussed with a doctor.
Contributed by: Department of Gynecologic Oncology, Gansu Wuwei Academy of Medical and Science
Contact Us
Consultation Hotline: 0935—2266423, 2267957
Address: Department of Gynecologic Oncology, 4th Floor, Outpatient Building, Gansu Wuwei Academy of Medical and Science

