
Contrast-Enhanced Ultrasound in the Diagnosis of Malignant Gallbladder Tumors
Contrast-Enhanced Ultrasound in the Diagnosis of Malignant Gallbladder Tumors
Contrast-enhanced ultrasound (CEUS), a new technology hailed as the "third revolution" in the history of ultrasound development, has been increasingly recognized and trusted by the clinical community, becoming an indispensable part of ultrasound diagnosis. Standing alongside CT and MRI, CEUS has emerged as one of the three major "sharp tools" for clinical disease diagnosis.
CEUS technology, based on conventional ultrasound, involves the bolus injection of a contrast agent (sulfur hexafluoride microbubbles) via the elbow vein to reach the lesion site. It enables real-time dynamic observation of blood perfusion in lesional tissues, providing a reliable basis for determining tumor nature, evaluating interventional therapeutic efficacy, and assessing treatment outcomes. CEUS examinations are convenient, fast, real-time dynamic, with immediate report availability, and short in duration. Additionally, the contrast agent used is a pure blood pool agent, characterized by small dosage, no need for skin testing, no hepatorenal damage, and excretion via the respiratory tract. It is particularly well-established in the diagnosis of focal hepatic lesions.
Our Department Case Review:
【Clinical Data】Female patient presented with upper abdominal distending pain without obvious predisposing cause one year prior to admission. She reported no nausea, vomiting, chills, high fever, acid reflux, diarrhea, jaundice of the skin/mucous membranes/sclera, hematemesis, or melena. Admitted to our hospital due to a "gallbladder space-occupying lesion" detected during an outpatient physical examination at another hospital. Laboratory tests showed normal results for six tumor markers.
【Conventional Ultrasound Imaging】The liver exhibited homogeneous echogenicity with no obvious space-occupying lesions. The gallbladder was normal in size and shape, with a thickened and rough wall. A 30×24mm hypoechoic mass was identified at the bottom of the gallbladder cavity, characterized by ill-defined margins, heterogeneous internal echogenicity, punctate hyperechoic foci, and strip-like blood flow signals. No dilation of the intrahepatic or extrahepatic bile ducts was observed, and no obvious abnormal echoes were detected in the visualized segments (Figure 1).
Abdominal cavity exploration: Several hypoechoic masses with well-defined margins and heterogeneous echogenicity were found adjacent to the abdominal aorta, containing short strip-like blood flow signals. The largest mass measured approximately 23×16mm (Figure 2).
Ultrasound findings: Solid space-occupying lesion within the gallbladder cavity (neoplastic lesion highly suspected; contrast-enhanced ultrasound recommended); Multiple hypoechoic masses adjacent to the abdominal aorta (enlarged lymph nodes highly suspected).

Figure 1 Hypoechoic mass at the bottom of the gallbladder cavity with strip-like blood flow signals inside.

Figure 2 Multiple enlarged para-aortic lymph nodes

Figure 3 High-frequency ultrasound shows the intact anterior wall of the gallbladder with no invasion of the liver.
【Contrast-enhanced ultrasound imaging】 As shown in Figures 4, 5, and 6.
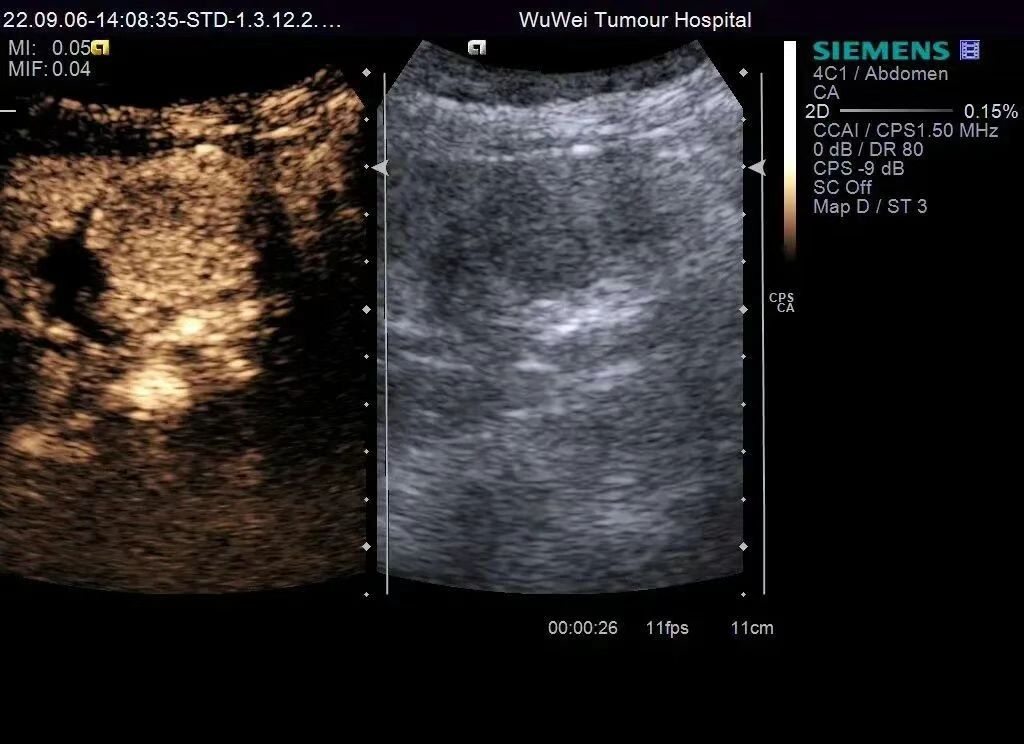
Figure 4 Contrast-enhanced ultrasound perfusion characteristics: The hypoechoic mass at the bottom of the gallbladder demonstrates homogeneous hyperenhancement higher than the surrounding liver parenchyma during the arterial phase, peaking at 20 seconds.
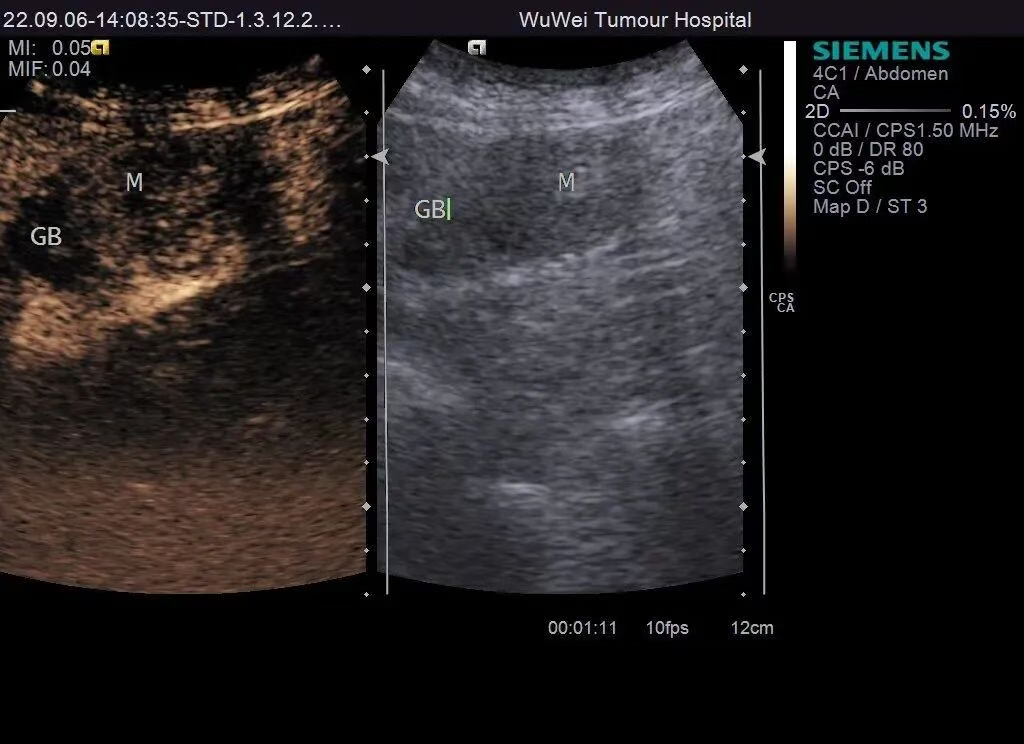
Figure 5 Contrast-enhanced ultrasound perfusion characteristics: The gallbladder lesion exhibits contrast agent washout at 49 seconds, with inhomogeneous hypo-enhancement during the portal venous phase.
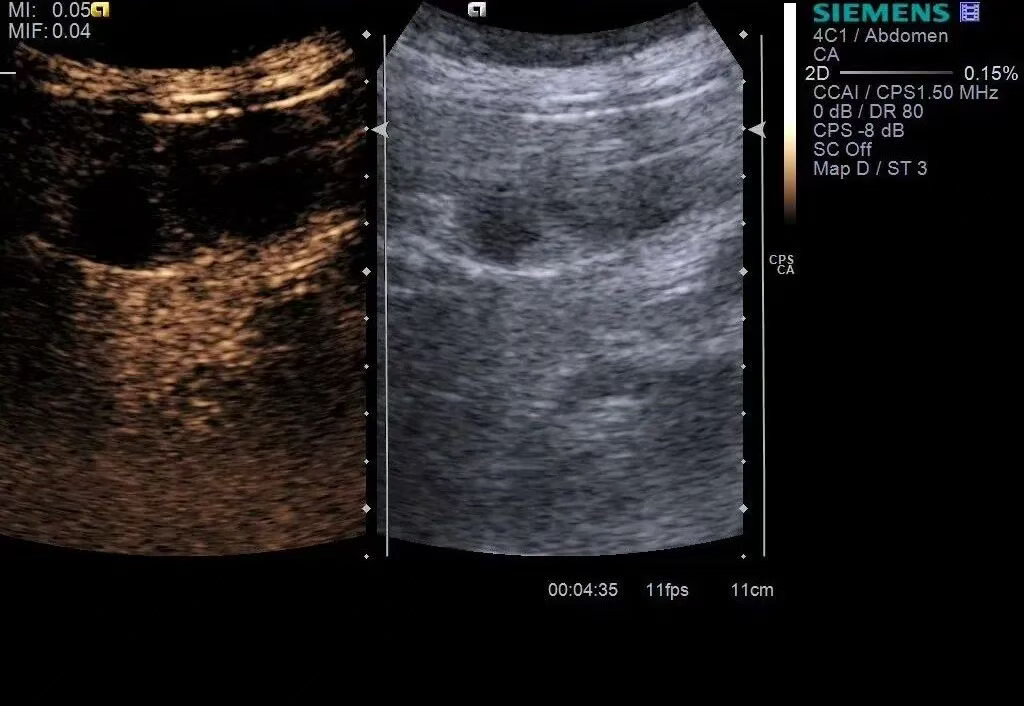
Figure 6 Contrast-enhanced ultrasound perfusion characteristics: The gallbladder lesion shows significant washout at 275 seconds, with persistent hypo-enhancement during the delayed phase.
【Surgical and Pathological Findings】Intraoperatively, the gallbladder was found to measure approximately 9×4 cm, with a firm mass (~2×2 cm) at its bottom that had extended beyond the serosal layer. Pathological results: Adenosquamous carcinoma at the gallbladder bottom; metastatic malignancy in the hepatic hilar lymph nodes. Cancerous tissue had penetrated the muscular layer of the gallbladder wall, with no invasion of the liver parenchyma. Invasion of lymphatic vessels, blood vessels, and nerves was observed. No cancerous tissue was detected at the cystic duct resection margin, but cancer metastasis was identified in the lymph nodes.
【Diagnostic Analysis】For this case, conventional ultrasound revealed a hypoechoic mass at the gallbladder bottom with internal blood flow signals and a clearly defined gallbladder wall structure. Contrast-enhanced ultrasound demonstrated a "rapid wash-in and rapid wash-out" enhancement pattern in the gallbladder bottom lesion, leading to a primary consideration of gallbladder carcinoma with metastasis to the hepatic hilar lymph nodes—findings consistent with the surgical and pathological results.
Preliminary Review: Zhang Jie
Final Review: Ma Shuqian