
Barrier Gel Enables Radical Heavy-Ion RT for Massive Tumor Thrombus
"Barrier Gel" Proves a Game-Changer: Radical Heavy-Ion Radiotherapy Achieved for Massive Vena Cava Tumor Thrombus
Recently, the Department of Radiation Oncology at the Lanzhou Branch of Gansu Wuwei Cancer Hospital successfully performed a laparoscopic "barrier gel implantation" between the duodenum and the inferior vena cava (IVC) for a patient with kidney cancer accompanied by a massive vena cava tumor thrombus. This innovative approach reduced the radiation dose to the duodenum to an extremely low level, allowing the IVC tumor thrombus to receive a curative dose of carbon-ion radiotherapy while avoiding severe radiation side effects. The case fully demonstrates the hybrid advantages of multidisciplinary collaboration and the integration of multiple advanced treatment techniques, turning clinical impossibilities into reality and bringing benefits to patients with advanced malignant tumors.
01 Critical Condition: Kidney Cancer + Massive IVC Tumor Thrombus (Extending into the Heart)
Mr. Xie, 36, sought medical attention due to visible hematuria and was diagnosed with left renal cell carcinoma accompanied by an IVC tumor thrombus. At diagnosis, the tumor was found to be large, and the thrombus extended upward along the IVC into the right atrium, making direct surgery unfeasible. Professor Ma Lulin administered six cycles of preoperative targeted-immunotherapy combination neoadjuvant treatment (tislelizumab + axitinib), achieving a partial response (PR) in efficacy evaluation. Follow-up MRI still suggested possible invasion of the vena cava wall by the tumor thrombus and involvement at the site where the hepatic veins drain into the vena cava—a worldwide challenge that current surgical methods cannot fully address. After discussing with the patient, a plan was made to perform "robot-assisted laparoscopic radical left nephrectomy + renal vein tumor thrombectomy + IVC tumor thrombus removal." During the surgery, it was discovered that the tumor thrombus had invaded the IVC wall up to the hepatic veins, leading to the decision to leave behind a portion of the renal vein and IVC tumor thrombus. The residual tumor thrombus was subsequently treated with radical heavy-ion radiotherapy.
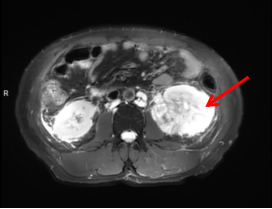
Figure 1 Preoperative MRI shows a large occupying lesion in the left kidney
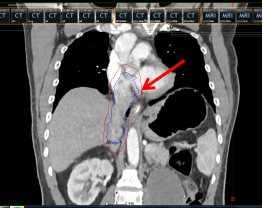
Figure 2 Tumor thrombus (area within the blue box indicated by the red arrow)
02 The Radiotherapy "Life-or-Death Challenge": Target Area Adjacent to Duodenum
Mr. Xie’s postoperative radiotherapy target area needed to cover: the left renal vein stump → inferior vena cava (IVC) → base of the right atrium. After patient positioning, Director Zhang Yingdong identified a critical issue during target delineation: part of the duodenum was directly adjacent to the tumor thrombus, making it impossible to avoid during radiotherapy. Administering carbon-ion therapy in this case would most likely cause severe intestinal ulceration, perforation, or bleeding—complications that could be life-threatening. Direct carbon-ion radiotherapy could not simultaneously achieve "tumor eradication" and "intestinal protection."
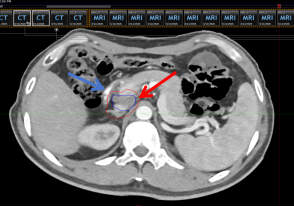
Figure 3 Positioning CT scan before barrier gel implantation (red arrow indicates the inferior vena cava target area, blue arrow indicates the duodenum)
03 Robust Protection: Implanting a Barrier Gel Between the Duodenum and Inferior Vena Cava
Faced with this radiotherapy challenge, Director Zhang Yingdong convened a multidisciplinary team (MDT) consultation for the complex case. Professor Wang Junjie, Director of the Radiation Oncology Department at Peking University Third Hospital and President of the Lanzhou Heavy-Ion Center, proposed a solution: drawing from the method used in radical carbon-ion radiotherapy for prostate cancer—where a barrier gel is implanted to protect the rectum—a barrier gel could be implanted between the IVC and the duodenum to safeguard the latter. Professor Ma Lulin from the Urology Department of Peking University Third Hospital noted that while there were no reported similar cases domestically or internationally, the procedure was technically feasible. "When facing a young, 37-year-old malignant tumor patient with the potential for curative treatment, we must have the courage to push boundaries," he emphasized.
✅ Three Key Roles of the Barrier Gel
1.Physical Separation: Pushes the intestine away from the high-dose radiation zone.
2.Positional Stabilization: Reduces displacement errors caused by breathing and peristalsis.
3.Safety Assurance: Significantly lowers the risk of radiation-induced gastrointestinal damage.
In simple terms, it acts like "protective armor" for the intestines, enabling radiotherapy to be delivered boldly, effectively, and safely.

Figure 4 Professor Ma Lulin and Director Zhang Yingdong discussing the heavy-ion radiotherapy plan for this patient
Figure 5 Schematic diagram of the "Laparoscopic Barrier Gel Implantation" procedure performed by Professor Ma Lulin
Once the treatment plan was finalized, Professor Ma Lulin, despite a long journey, immediately began preoperative preparations with Dr. Yang Yun from the Urology Department of Wuwei Cancer Hospital at the Lanzhou Heavy-Ion Center for the "Laparoscopic Barrier Gel Implantation" surgery. The procedure commenced at 8 PM that same day. Professor Ma, utilizing laparoscopy, adopted a retroperitoneal approach through the lower right abdomen. He carefully dissected the fascial plane between the ventral side of the right kidney/IVC and the dorsal side of the duodenum, then injected the barrier gel into the created space. The patient returned to the ward in stable condition after the operation.
Following the barrier gel implantation, a repeat positioning scan prior to carbon-ion therapy revealed that the duodenum was now separated from the IVC by approximately 3 cm—far exceeding the 8 mm safety distance required for carbon-ion radiotherapy targets to clear critical organs.
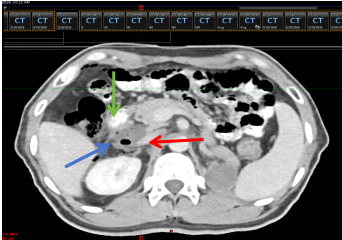
Figure 6 Positioning CT scan after barrier gel implantation
(Red arrow indicates the inferior vena cava, green arrow indicates the duodenum, blue arrow indicates the barrier gel)
The patient recovered well postoperatively and began the first course of carbon-ion therapy one week later, with a dose of 36 Gy(RBE) in 9 fractions of 4 Gy(RBE) each. A follow-up CT scan after this first course showed significant regression of the tumor thrombus; its upper border had receded from the right atrium down to the level of the hepatic vein confluence. The patient has now begun a second course of carbon-ion therapy in the prone position. Throughout the treatment, he has experienced no gastrointestinal radiation side effects. The total planned dose for both courses is 72 Gy(RBE), completing the radical carbon-ion radiotherapy for the residual IVC tumor thrombus after nephrectomy.
This pre-radiotherapy barrier gel implantation fully exemplifies the rigor and precision of our hospital's carbon-ion therapy, always prioritizing patient safety and benefit.
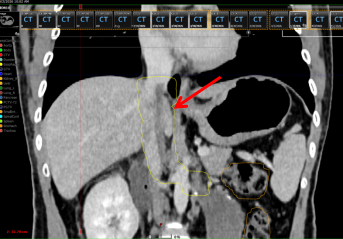
Figure 7 Tumor thrombus regression after the first course of treatment
(Area within the yellow box indicated by the red arrow)
Key Experts
Zhang Yingdong
Chief Physician, Director of the Third Department of Radiation Oncology at the Lanzhou Branch of Gansu Wuwei Cancer Hospital. Former administrative head of the Radiation Oncology Department at Peking University International Hospital, and a postgraduate in Oncology Radiotherapy from Peking University Third Hospital. He serves as a committee member of the Radiation Therapy Professional Committee of the Bethune Charitable Foundation, a member of the Central Nervous System Tumor Radiotherapy Group under the Radiation Oncologist Branch of the Chinese Medical Doctor Association, a committee member of the Tumor Radiotherapy Professional Committee of the Beijing Anti-Cancer Association, and a committee member of the Head and Neck Tumor MDT Professional Committee of the Beijing Cancer Prevention and Control Society. With over 30 years of experience in tumor radiotherapy, he specializes in radiation therapy for malignant tumors of the central nervous system, head and neck, chest, abdomen, pelvis, and limbs, and has conducted in-depth research on combined treatments such as chemotherapy, targeted therapy, and immunotherapy during radiotherapy.

Professor Wang Junjie
Doctoral Supervisor, Chief Physician, President of the Lanzhou Branch of Gansu Wuwei Cancer Hospital, and former Chairman of the 10th National Radiotherapy Committee of the Chinese Medical Association. He is also the Director of the Radiation Oncology Department at Peking University Third Hospital. His roles include standing committee member of the Tumor Minimally Invasive Treatment Committee of the Chinese Anti-Cancer Association, head of the Particle Therapy Group, committee member of the Interventional Therapy Professional Committee of the Chinese Anti-Cancer Association, standing committee member of the Geriatric Oncology Professional Committee of the Chinese Geriatrics Society, Vice Chairman of the Beijing Society for Radiation Oncology, council member of the Beijing Anti-Cancer Association, committee member of the Radiation Oncology Expert Committee of the Beijing Medical Doctor Association, and President of the Lanzhou Heavy-Ion Center at Gansu Wuwei Cancer Hospital. He specializes in tumor radiotherapy, chemotherapy, targeted therapy, and immunotherapy, with particular expertise in lung nodule puncture, three-dimensional stereotactic radiotherapy (CyberKnife), radioactive seed implantation, and comprehensive treatment for head and neck tumors, lung cancer, liver cancer, pancreatic cancer, prostate cancer, and soft tissue tumors.

Professor Ma Lulin
Former Director of the Urology Department at Peking University Third Hospital, Chief Physician, Doctoral Supervisor, Postdoctoral Co-Supervisor, Peking University Second-Level Professor, and Vice President of the Haidian Branch of Peking University Third Hospital. He began his career in urology in 1984 and is a nationally renowned urology expert. He is highly skilled in kidney transplantation, living-related kidney transplantation, and combined pancreas-kidney transplantation. He excels in open surgery, laparoscopic-assisted, and robot-assisted complex urological procedures, including resection of large adrenal tumors, radical prostatectomy for kidney cancer with vena cava tumor thrombus, radical prostatectomy, total cystectomy with orthotopic neobladder, ileal conduit, and ureterocutaneostomy. He also has profound expertise in laparoscopic surgeries such as kidney transplantation, nerve-sparing radical prostatectomy, nerve-sparing total cystectomy with lymph node dissection and Studer orthotopic neobladder, radical nephrectomy, partial nephrectomy, and resection of large adrenal tumors.