
3 cases of orbital malignant tumor treated with carbon ion radiotherapy and literature review
3 cases of orbital malignant tumor treated with carbon ion radiotherapy and literature review
LU Jing, LI Xiao-jun*, CHAI Hong-yu, WANG Yan
Department of Heavy Ion Radiotherapy, Lanzhou Branch of Wuwei Cancer Hospital of Gansu, Lanzhou, Gansu, 730000, China
ABSTRACT Objective: To investigate the efficacy and safety of carbon ion radiotherapy (CIRT) in 3 cases of orbital malignant tumors. Methods: The clinical data of 3 patients with orbital malignant tumor who received CIRT treatment in Wuwei Cancer Hospital of Gansu Province from July 2022 to July 2023 were retrospectively analyzed, and the relevant literature was reviewed. Results: Three patients completed CIRT treatment, they were followed up for an average of 20.5 months (15-26 months). Case 1 achieved complete response (CR) 3 months after CIRT treatment, case 2 achieved CR 3 months after CIRT treatment, and case 3 achieved partial response (PR) 12 months after CIRT treatment. The 1 year local control rate (LC), 1-year progression-free survival (PFS), and 1-year overall survival (OS) of the three patients were 100.0%. One patient had grade 1 radiation conjunctival injury, 2 patients had grade 1 radiation skin reaction, and 1 patient had grade 1 dry eye late adverse reaction. No adverse reactions of grade 2 or higher occurred in all patients. Conclusion: The application of CIRT in unresectable, postoperative residual and recurrent orbital malignant tumors can obtain good OS and LC, and acute and late toxic reactions are less.
Key words: Carbon ion radiotherapy; Orbital malignant tumor; Curative effect
Introduction
Orbital malignant tumours of the eye originating in the orbit have an incidence of 3.4/106 persons/year, accounting for 0.1% of all tumours and less than 20% of all ocular diseases [1-2]. Orbital anatomy is complex, and intraorbital tissues can originate from epidermal ectoderm, mesoderm and neural ectoderm, etc. Therefore, orbital malignant tumours are varied and complicated to classify, and the disease progresses rapidly, which not only affects the patient's vision and appearance, but also may have distant metastasis or even lead to the patient's death [3-4]. Surgery is the main treatment for orbital malignant tumours, and complete resection of orbital malignant tumours is more difficult to achieve due to positive or subcutaneous surgical margins, positive lymph nodes, perineural infiltration, and locally advanced tumours, etc. Therefore, for patients with orbital malignant tumours after surgery and for those who are unable to undergo surgical resection, radiotherapy, chemotherapy, and other comprehensive treatments are usually given [5-6]. Intensity-modulated radiotherapy (IMRT) is a commonly used adjuvant treatment for postoperative patients with orbital malignancies and those who cannot undergo surgical resection, but radiotherapy-induced toxicity limits the dose of IMRT to the tumour target, and affects efficacy due to the high dose at the entrance and exit of the beam path, which results in difficulty in covering the tumour dose and in making the volume of the surrounding normal tissues higher in dose [7]. Low doses are usually insufficient to control common orbital malignancies including squamous cell carcinoma, adenoid cystic carcinoma (ACC) and soft tissue sarcoma (STS) [8]. Therefore, there is a need to explore a more effective treatment technique with lower side effects to break the current bottleneck in the treatment of orbital malignancies. In this study, we retrospectively analysed the clinical data of three patients with orbital tumours and the efficacy and safety of treatment with carbon ion radiotherapy (CIRT), and reviewed the relevant literature to deepen the understanding of this treatment modality and its efficacy.
1. Clinical information
Case 1: Female, 44 years old, squamous carcinoma of the right lacrimal sac. She visited our hospital in July 2022, and on examination, she was found to have a swelling of about 3 cm × 4 cm in size in the lower eyelid of her right eye, with mild limitation of eye movement in all directions. After a thorough examination and evaluation of the patient, the patient was treated on 20 July 2022 with CIRT. The prescribed dose for the first course: PTV 40Gy (RBE)/10fx; lateral position, 2D homogeneous scanning, and the dose distribution is shown in Figure 1A.The prescribed dose for the second course: PTVboost 24Gy (RBE)/6fx; supine position, 2D homogeneous scanning. The total dose to the tumour area was 64 Gy (RBE)/16 F, 4.0 Gy (RBE)/F, and 5 F/w, and the dose distribution is shown in Fig. 1B.Comparison of the dose distribution of axial images between CIRT and volume-modulated intensity-adjusted radiotherapy (VMAT) plans while both fulfilling the prescriptive requirements, and the range of the surrounding normal tissues irradiated at low doses was significantly smaller for the CIRT plan compared to the VMAT plan, see Fig. 2A and The efficacy of CIRT was compared by imaging data before and after treatment, and the patient's efficacy was assessed according to the Response to Evaluation Criteria for the Evaluation of Solid Tumours (RECIST) 1.1, and the efficacy of treatment reached a complete remission (CR) 3 months after treatment, as shown in Fig. 3. During the CIRT treatment period and in the first month after the treatment, the patient developed grade 1 acute radiation conjunctival injury; 3 months after the end of radiotherapy, she developed dry eyes, and the use of eye drops for a long time was considered to be grade 1 radiation conjunctival damage, which was considered to be grade 1 radiation conjunctival damage. , considered grade 1 radiation conjunctival injury (RTOG Acute Radiation Injury Grades), no late adverse events greater than grade 2 were observed.Combination of a target (cetuximab) during CIRT treatment, with disseminated rash on the face during the treatment period, grade 1 on the Common Terminology Evaluation Criteria for Adverse Events. As of September 2024, the patient is currently disease-free and continues to be followed for the long term.
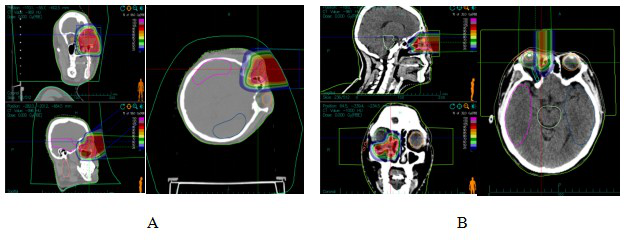
Figure 1 CIRT dose distribution in patients with dacryocystosquamous cell carcinoma
Note: Figure 1A: One course CIRT dose distribution. Figure 1B: Two course CIRT dose distribution
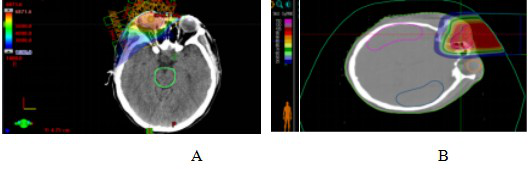
Figure 2 VMAT plan and carbon ion plan dose distribution in patients with dacryocystosquamous cell carcinoma
Note: Figure 2A: VMAT plan dose distribution in patients with dacryocystosquamous cell carcinoma. Figure 2B: Carbon ion plan dose distribution in patients with dacryocystosquamous cell carcinoma.
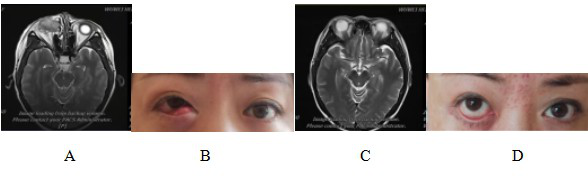
Figure 3 Comparison of magnetic resonance imaging (MRI) and physical signs in patients with dacryocystosquamous cell carcinoma before and after CIRT treatment
Note: Figure 3A: MRI examination before CIRT treatment showed that: the right lacrimal sac was occupied, the boundary between the eyeball, the medial rectus muscle and the inferior rectus muscle was not clear, the eyeball was compressed and displaced, and the right nasolacrimal duct was invaded. Figure 3B: Abnormal signs before CIRT treatment; Figure 3C: MRI examination after CIRT treatment showed that: the lesion disappeared, and the efficacy evaluation was CR; Figure 3D: Recovery of physical signs after CIRT treatment.
Case 2: Male, 38 years old, malignant melanoma of the choroid of the right eye. He presented to our hospital in April 2023 with a funduscopic examination that showed a clear and reddish optic disc border, a brownish-black highly elevated mass visible in the temporal inferior quadrant of the retina, and secondary retinal detachment in the periphery of the mass, which was spreading to the macular area. The patient was treated with CIRT from 25 April to 12 May 2023 after a thorough examination and evaluation. The prescribed dose was PTV 70Gy/14Fx, 5GyE/Fx. Supine position, 2D uniform scanning technique, dose distribution is shown in Fig. 4. Typical comparison of dose distribution in axial images between CIRT and VMAT plans while both fulfilling the prescription requirements, peripheral normal tissues were significantly reduced in the range of low-dose irradiation for the CIRT plan compared to the VMAT plan, as shown in Fig. 5. During the treatment period the patient was given Teraplizumab injection (240 mg) for 2 cycles of immunotherapy.The efficacy of CIRT was compared by imaging data before and after treatment, and the patient's efficacy was assessed according to the RECIST1.1 criteria for evaluating oncological efficacy, and the efficacy of the treatment was a CR at 3 months post-treatment, as shown in Fig. 6.During the period of CIRT treatment and 1 month post-treatment, the patient experienced grade 1 radioskin lesions, with the same visual acuity as before, and no greater than grade 2 adverse events, and visual acuity improved 3 months after treatment. As of September 2024, the patient is currently disease-free and continues to be followed up on a long-term basis.
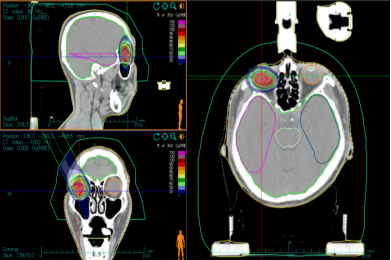
Figure 4 CIRT dose distribution in patients with malignant choroidal melanoma
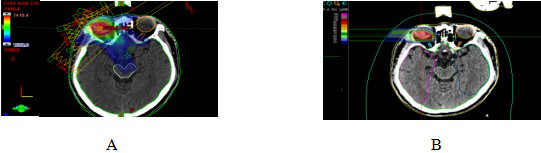
Figure 5 VMAT plan and carbon ion plan dose distribution in patients with malignant choroidal melanoma
Note: Figure 5A: VMAT plan dose distribution in patients with malignant choroidal melanoma. Figure 5B: Carbon ion plan dose distribution in patients with malignant choroidal melanoma.
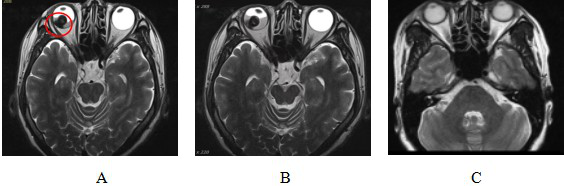
Figure 6 Comparison of MRI before and after CIRT treatment for malignant melanoma of choroid
Note: Figure 6A: MRI examination results before CIRT treatment showed: Abnormal signal nodules on the right side of the base of the eyeball. The red circle shows the extent of tumor invasion.
Figure 6B: MRI results after CIRT treatment showed: Abnormal signal nodules on the right lateral temporal side of the base of the eyeball, with little change compared with before.
Figure 6C: MRI examination 90 days after CIRT treatment showed that: the lesion disappeared and the efficacy was evaluated as CR.
Case 3: Female, 59 years old, postoperative right orbital ACC. She underwent ‘right orbital mass excision + orbital repair’ at West China Hospital of Sichuan University in April 2023, and her postoperative examination showed that she had ACC. she was admitted to our hospital one month after the operation, and now she has obvious limitations in eyelid closure, right eye external rotation and downward rotation. After a thorough examination and evaluation of the patient, the patient was treated with CIRT on 12 June 2023, with one prescribed dose of PTVboost: 15Gy (RBE)/5fx. the second prescribed dose was PTV: 54Gy (RBE)/18fx, and the total tumour dose amounted to 69Gy (RBE)/23fx, with the dose distribution shown in Fig. 7. the CIRT and VMAT plans, under the premise that both meet the prescription requirements, the typical comparison of dose distribution in axial images, the surrounding normal tissue CIRT plan is significantly smaller than the VMAT plan low-dose irradiation range, see Figure 8.The efficacy of CIRT treatment was compared by imaging data before and after treatment, and the patient's efficacy was assessed according to the RECIST1.1 criteria for evaluating the effectiveness of tumour efficacy, which reached a partial remission (PR), see Figure 9. During CIRT treatment and within 1 month after treatment, the patient experienced grade 1 radioskin injury, and no adverse events greater than grade 2 were observed. As of July 2024, the patient is currently surviving with tumour and continues to be followed up in the long term.
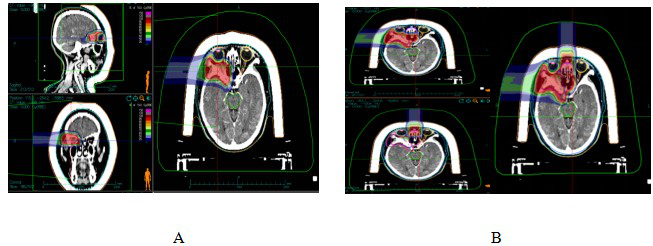
Figure 7 Ion therapy dose distribution in orbital ACC patients
Note: Figure 7A: One course CIRT dose distribution. Figure 7B: Two course CIRT dose distribution
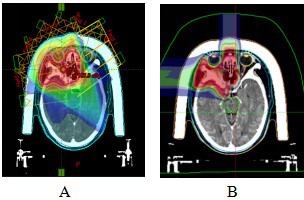
Figure 8 VMAT plan and carbon ion plan dose distribution in orbital ACC patients
Note: Figure 8A: VMAT plan dose distribution n orbital ACC patients. Figure 8B: Carbon ion plan dose distribution n orbital ACC patients.
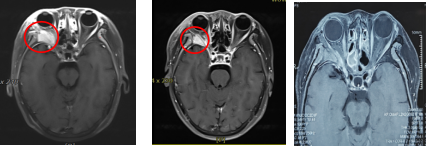
Figure 9 Comparison of MRI before and after CIRT treatment for orbital ACC patients
Note: Figure 9A: MRI examination before CIRT treatment showed that: the right orbital space was occupied, and the boundary between the right orbital muscle and the external rectus muscle, lacrimal gland, and optic nerve was unclear, and the lateral wall of the orbit was invaded.
Figure 9B: MRI examination after CIRT treatment showed that: the right orbital space was occupied and abnormal enhancement, and the lateral orbital wall was invaded, which was smaller than that of the anterior lesion. The efficacy evaluation was PR.
Figure 9C: MRI examination 12 months after CIRT treatment showed that: the right orbital space was significantly reduced compared with the anterior lesion, and the efficacy evaluation was PR.
2. Results
2.1 Evaluation of therapeutic efficacy
The average follow-up period of the 3 cases was 20.5 months (15-26 months). Case 1 dacryocystic squamous carcinoma patient reached CR immediately after CIRT, Case 2 choroidal malignant melanoma patient reached CR at 3 months after treatment, and Case 3 orbital ACC patient is currently being followed up to 1 year to reach PR. 1-year progression-free survival (PFS) rate of the 3 patients was 100.0%, 1-year local control (LC) rate was 100.0%, and 1-year overall survival (OS) rate was 100.0%.
2.2 Safety evaluation
No grade ≥2 radiotherapy-related adverse reactions occurred in all patients. Acute-phase reactions occurred mostly during treatment and within 1 month after treatment, and manifested as radioskin reactions and eye injuries. grade 1 radioconjunctival injury occurred in 1 case, which manifested as mild conjunctivitis with conjunctival congestion, and grade 1 radioskin reactions occurred in 2 cases, which manifested as skin hyperpigmentation in irradiated fields with small flaky erythema. In terms of late adverse reactions, one case of radioactive conjunctival damage was observed, which manifested itself as dry eyes and required long-term use of eye drops, and occurred three months after the end of radiotherapy.
Discussion
Orbital tumours are a heterogeneous group of lesions with different classifications, histological features, diagnostic criteria, treatment methods and survival rates. Its histopathology is complex, due to the differences in biological behaviours, different sensitivity to radiotherapy and chemotherapy, and different clinical prognosis, some of which are prone to local or regional recurrence, and some of which are prone to early distant metastasis, so there are differences in clinical treatment methods [9-11].
The treatment methods for orbital malignant tumours include surgery, adjuvant radiotherapy, intervention, chemotherapy, targeted and immunotherapy, etc. Orbital surgery has the characteristics of narrow space, concentration of important tissue structures, and narrow surgical field, therefore, it is difficult to perform surgery, and there are many postoperative complications [12-13]. Radical surgery is usually difficult to achieve in patients with orbital malignant tumours due to the inability to obtain adequate margins for eye preservation. Radiotherapy for patients with orbital tumours is still dominated by photon therapy, but most orbital tumours (e.g., ACC, retinoblastoma, malignant melanoma, sarcoma, etc.) often recur locally after photon radiotherapy. In one study, 39 patients with orbital malignancies were treated surgically, of whom approximately 20% developed local recurrence after a median follow-up of 8 months, with 3-year OS and recurrence-free/death-free survival rates of 50.5% and 47.5%, respectively [14].
In recent years, with the advancement of medical technology, some new radiotherapy techniques such as proton and carbon ion have come into the limelight. In a study [15], 22 patients with orbital tumours who underwent proton radiotherapy (PRT) and/or CIRT after eye-sparing surgery had 2-year OS, PFS, and distant metastasis-free survival (DMFS) rates of 100%, 57.9%, and 72.8%, respectively; no acute severe (i.e., grade ≥3) toxicity was observed, and the incidence of severe late toxicity was rare. In addition, BED (biological effect dose) may have a significant effect on DMFS (distant metastasis-free survival): the higher the BED, the lower the risk of distant metastasis. These findings suggest that particle therapy may have a significant impact on disease control. Higher BED was found to be associated with improved outcomes in the study, suggesting that the advantages of CIRT treatment are usually reflected in the fact that the tumour dose can be increased based on dose limitation to neighbouring critical organs, without increasing the incidence of toxic reactions [16].
Studies have shown that with radiotherapy doses over 50 Gy, the conjunctiva is keratinised and the lacrimal glands show atrophy, fibrosis and corneal decompensation. When doses exceed 60 Gy, lid adhesions, keratoconjunctivitis, and chronic dry eyes become a problem. In addition, radiation-induced optic neuropathy may occur in about 7.0%-20.0% of patients [17-19]. Carbon ion beams can concentrate the dose within the target tissue by forming Bragg peaks through energy deposition, killing the tumour cells in the target area while protecting as much as possible the normal tissues in the surrounding area and on the radiation pathway to minimize the damage [20-22]. A study showed [23] that the heavy ion beam is located at the edge of the target area due to its unique physical properties, the dose drop is very rapid, and the trailing edge of the heavy ion beam can be attenuated by 70%~80% at a distance of 5 mm from the 95% isodose line, and the dose can be attenuated by about 8%~19% at a distance of 1 mm from the trailing edge of the shot field. Therefore, carbon ions are suitable for safe and adequate radiotherapy in some target areas adjacent to critical organs [24-25].
There are some limitations to this study. Firstly, orbital tumours comprise a heterogeneous group of conditions of different origins with essentially different biological behaviours, and the combination of different pathologies inevitably affects the uniformity of the results. Second, the follow-up time was limited, so this study will continue to follow these patients and observe the prognosis at long-term follow-up. Thirdly, two patients in this study were scanned uniformly and one patient was scanned with a spot scan, which may differ in terms of the amount of endangered organs received and toxic side effects. In uniform scanning, a tissue compensator is needed to remove the dose falling behind the tumour through the adjustment of the compensator, but some normal tissues on the incident path of the carbon ion beam will inevitably be irradiated with a certain dose; with carbon ion spot scanning, the depth of the ion beam is changed by changing the energy of the particles, and a three-dimensional conformal scanning is carried out for the target area of the tumour by using a pen-shaped beam, and the area of high-dose distribution (Bragg peak) is adjusted to be embedded in the target area of the tumour, and the high dose distribution area is adjusted to be embedded in the target area of the tumour. The high dose distribution area (Bragg peak) is adjusted to be embedded in the tumour target area, the dose at the trailing edge of the shot field falls rapidly, and the difference in RBE value between the peak area and the ping area is the largest, which further reduces the dose of the neighbouring organs at risk located in the ping area. Fourth, the first domestic heavy ion therapy with a fixed field path and few field directions (vertical and horizontal) failed to give full play to the advantages of carbon ions, and the 45° field will be put into use soon, which is expected to provide more possibilities for the precise treatment of head and neck tumours, especially orbital tumours. Fifth, this study is a retrospective study with a relatively small sample size, and considering the rarity of this disease, almost all of the current published literature comes from retrospective studies at a single institution. Without collaboration between specialised academic centres, it would be difficult to conduct prospective studies to explore the efficacy of different treatment modalities or techniques.
In summary, the three cases of CIRT for orbital malignancies reported in our centre achieved satisfactory 1-year OS, LC and PFS rates, and no serious acute or late toxic reactions were observed. For inoperable, residual postoperative, and postoperative recurrent orbital malignancies, CIRT carbon ion radiotherapy is an efficacious.
Reference
[1]Pol JN, Patil DB, Desai SS, et al. Malignant recurrent orbital solitary fibrous tumor[J]. Indian J Pathol Microbiol, 2023, 66(4):819-822.
[2]Biswas A, Kumar R, Bakhshi S, et al. Multimodal Management of Congenital Orbital Malignant Rhabdoid Tumor: Review of Literature and Report of a Rare Case[J]. J Pediatr Hematol Oncol, 2020, 42(3):228-233.
[3]Poudyal P, Hamal D, Shrestha P. Orbital Tumors and Tumor like Lesions: A Hospital Based Study[J]. J Nepal Health Res Counc, 2022, 20(1):26-32.
[4]Tom A, Bell D, Ford JR, et al. Malignant Mixed Tumor (Carcinoma Ex Pleomorphic Adenoma) of the Lacrimal Gland[J]. Ophthalmic Plast Reconstr Surg, 2020, 36(5):497-502.
[5]Joseph AK, Guerin JB, Eckel LJ, et al. Imaging Findings of Pediatric Orbital Masses and Tumor Mimics[J]. Radiographics, 2022, 42(3):880-897.
[6]Jones KE, Patel A, Kunesh MG, et al. Malignant peripheral nerve sheath tumor of the orbit: a case report and review of the literature[J]. Orbit, 2022, 41(5):642-646.
[7]Chen X, Badian RA, Hynne H, et al. Alterations in meibomian glands in patients treated with intensity-modulated radiotherapy for head and neck cancer[J]. Sci Rep, 2021, 11(1):22419.
[8]Wu F, Chen B, Dong D, et al. Phase 2 Evaluation of Neoadjuvant Intensity-Modulated Radiotherapy in Centrally Located Hepatocellular Carcinoma: A Nonrandomized Controlled Trial[J]. JAMA Surg, 2022, 157(12):1089-1096.
[9]Reshef ER, Bleier BS, Freitag SK. The Endoscopic Transnasal Approach to Orbital Tumors: A Review[J]. Semin Ophthalmol, 2021, 36(4):232-240.
[10]Ye-Zhu C, Muñoz-Ramón PV, Barrancos C, et al. Orbital myopericytoma: an unusual tumor in an unusual location[J]. Orbit, 2022, 41(4):502-505.
[11]Tooley AA, Maher M, Cooper C, et al. Reliability of 3 Strategies of Orbital Tumor Volume Measurement Using Phantom Modeling[J]. Ophthalmic Plast Reconstr Surg, 2021, 37(3S):S33-S38.
[12]Zhou Q, Liu Y, Wang F, et al. A giant orbital solitary fibrous tumor treated by surgical excision: a case report and literature review[J]. Diagn Pathol, 2023, 18(1):59.
[13]Feu-Basilio S, Matas J, Dotti-Boada M, et al. Orbital TFE3-Rearranged Perivascular Epithelioid Cell Tumor: A Case Report and Review of the Literature[J]. Am J Dermatopathol, 2021, 43(12):e263-e266.
[14]Orapan Aryasit, Passorn Preechawai, Chakree Hirunpat, et al. Factors related to survival outcomes following orbital exenteration: a retrospective, comparative, case series[J]. BMC Ophthalmol, 2018, 18(1):186.
[15]Aki Hirai, Atsushi Mizota, Seiichiro Mine, et al. Two cases of orbital adenocarcinoma treated with heavy charged carbon particle irradiation[J]. Graefes Arch Clin Exp Ophthalmol, 2005, 243(6):610-614.
[16]Huang SF, Lin JC, Shiau AC, et al. Optimal tumor coverage with different beam energies by IMRT, VMAT and TOMO: Effects on patients with proximal gastric cancer[J]. Medicine (Baltimore), 2020, 99(47):e23328.
[17]Pointreau Y, Moreau J, Vendrely V, et al. Impact of IMRT for neoadjuvant rectal cancer?[J]. Cancer Radiother, 2022, 26(6-7):865-870.
[18]Itonaga T, Mikami R, Okubo M, et al. Prognostic impact of solid tumor component diameter in early-stage non-small cell lung carcinoma treated with intensity-modulated fractionated radiotherapy: a retrospective analysis impact of solid tumor component diameter in NSCLC treated with IMRT[J]. Br J Radiol, 2020, 93(1109):20191027.
[19]Liu X, Wu B, Huang J, et al. Tumor factors associated with in-field failure for nasopharyngeal carcinoma after intensity-modulated radiotherapy[J]. Head Neck, 2022, 44(4):876-888.
[20]Killock D. Recurrent nasopharyngeal carcinoma: hyperfractionation of IMRT improves outcomes[J]. Nat Rev Clin Oncol, 2023, 20(5):283.
[21]Takahashi D, Demizu Y, Koto M, et al. Multicenter study of re-irradiation using carbon-ions for head and neck malignancies after photon radiotherapy[J]. Cancer Med, 2022, 11(19):3593-3601.
[22]Liu X, Yue H, Jiang S, et al. Clinical features and prognosis of patients with metastatic ocular and orbital melanoma: A bi-institutional study[J]. Cancer Med, 2023, 12(15):16163-16172.
[23]Susko MS, Lazar AA, Dhar S, et al. Improved Tumor Control Related to Radiotherapy Technological Development for Hypopharyngeal Cancer[J]. Laryngoscope, 2021, 131(2):E452-E458.
[24]陈宇鹏, 史路林, 王瑜玉, 等. GeV重离子束辐照LiF引起的晶体内部结构改变[J]. 物理学报, 2024, 73(15):111-117.
[25]Shih CY, Huang WL, Chiang IT, et al. Biocompatible hole scavenger-assisted graphene oxide dots for photodynamic cancer therapy[J]. Nanoscale, 2021, 13(18):8431-8441.

