
Breast Cancer Carbon Ion Radiotherapy: Exploring a Radical Alternative to Surgery
Breast Cancer Carbon Ion Radiotherapy: Exploring a Radical Alternative to Surgery
Breast cancer is the most common tumor among women worldwide, posing a serious threat to women's life and health, and is the sixth leading cause of cancer death among Chinese women.
In recent years, the incidence of breast cancer in China has been continuously rising, and an increasing number of young people are developing breast cancer. According to 2018 statistics, globally, China ranked first in breast cancer incidence among 154 countries and first in mortality among 104 countries. The rapid development of medical technology has enabled more patients to be diagnosed at an early stage of the disease. Radical mastectomy was established by Halsted in 1882, and surgical treatment still plays an important role in breast cancer therapy. Surgery remains the primary treatment, followed by radiotherapy, chemotherapy, endocrine therapy, and targeted therapy, which are the main current approaches for treating breast cancer.
Non-surgical treatments for breast cancer are currently in the exploratory stage, including radiofrequency ablation, cryoablation, stereotactic body radiation therapy (SBRT), and carbon ion radiotherapy (CIRT). These modalities provide alternative treatment options for patients unwilling or unable to undergo surgery. However, these local treatments are currently only suitable for microinvasive cancers with tumor sizes <2 cm. The safety and efficacy of carbon ion therapy for breast cancer treatment require further exploration.
This article shares one typical case of breast cancer treated with the Wuwei Carbon Ion Therapy System, aiming to provide a reference for clinical research on carbon ions as an alternative to surgery for breast cancer.
Clinical Data
Patient: Female, 44 years old.
Chief Complaint: "Discovered a mass in the right breast for 7 months" admitted on 2020-05-30. Seven months prior to admission, the patient accidentally discovered a painless mass measuring 3 cm×3 cm in the outer lower quadrant of the right breast, which she did not pay much attention to. In March 2020, the patient experienced intermittent needle-like pain in the right breast. Further ultrasound examination indicated: a hypoechoic nodule visible in the right breast, biopsy recommended.
Right breast core needle biopsy was performed. Postoperative pathology indicated: Invasive carcinoma of no special type. Immunohistochemistry (IHC): CK (+), ER (+, 40%, weak-moderate), PR (+, 30%, weak), Her-2 (1+), P63 (−), CR5/6 (−), E-cad (+), Ki-67 (+, 50%).
The patient received traditional Chinese medicine treatment orally. One month later, a follow-up breast ultrasound showed the mass had slightly enlarged compared to the previous examination. Due to personal religious beliefs, the patient was unwilling to undergo surgery that would result in organ loss and refused surgical treatment. She was admitted on 2020-05-30 and hospitalized under the diagnosis of "Malignant tumor of the breast".
During the course of illness, the patient was conscious, in fair spirits, with normal diet, good sleep, and normal bowel and bladder function. Past history: Denied history of "hypertension," "heart disease," "diabetes," "cerebrovascular disease," and infectious diseases such as "hepatitis," "tuberculosis," "malaria." Underwent "cesarean section" at a local hospital in 2009. No history of trauma, blood transfusion, or food or drug allergies. No history of smoking or alcohol consumption. No history of extramarital affairs. Menarche at age 13, menstrual cycle 21~25 days, duration of menstruation 2~5 days, last menstrual period on 2020-05-07. Sister has breast cancer.
Physical Examination: A 1 cm×1 cm enlarged lymph node palpable in the right axilla, with clear boundaries, firm consistency, good mobility, and no tenderness. A 3 cm×3 cm mass palpable in the outer lower quadrant of the right breast, with clear boundaries, firm consistency, good mobility, and no tenderness.
Examinations
Breast Color Doppler Ultrasound: Solid mass in the right breast, enlarged lymph nodes in the right axilla. Chest CT: Abnormally enhancing nodule/mass shadow in the right breast, highly suggestive of breast cancer (2.5 cm×1.7 cm); Enlarged lymph node in the right axilla, largest approximately 1.2 cm×0.6 cm; Several small lymph nodes in bilateral axillae.
Pathology after right breast biopsy indicated: Invasive carcinoma of no special type. Immunohistochemistry: CK (+), ER (+, 40%, weak-moderate), PR (+, 30%, weak), Her-2 (1+), P63 (−), CR5/6 (−), E-cad (+), ki-67 (+, 50%).
Diagnosis and Differential Diagnosis
Diagnosis: Based on the patient's pathological examination results, a clear diagnosis of invasive carcinoma of the right breast was made, staged as cT2N1Mx Stage IIB (AJCC 8th Edition). The pathological diagnosis is definitive, no differential diagnosis required.
Treatment
The patient refused surgery and was admitted. Carbon ion therapy was administered to the right breast mass, right axillary metastatic lymph node, right chest wall, and the lymphatic drainage areas of the right axilla and supraclavicular region. The dose was 72 Gy (RBE)/12 Fx (Fig 1, Fig 2).
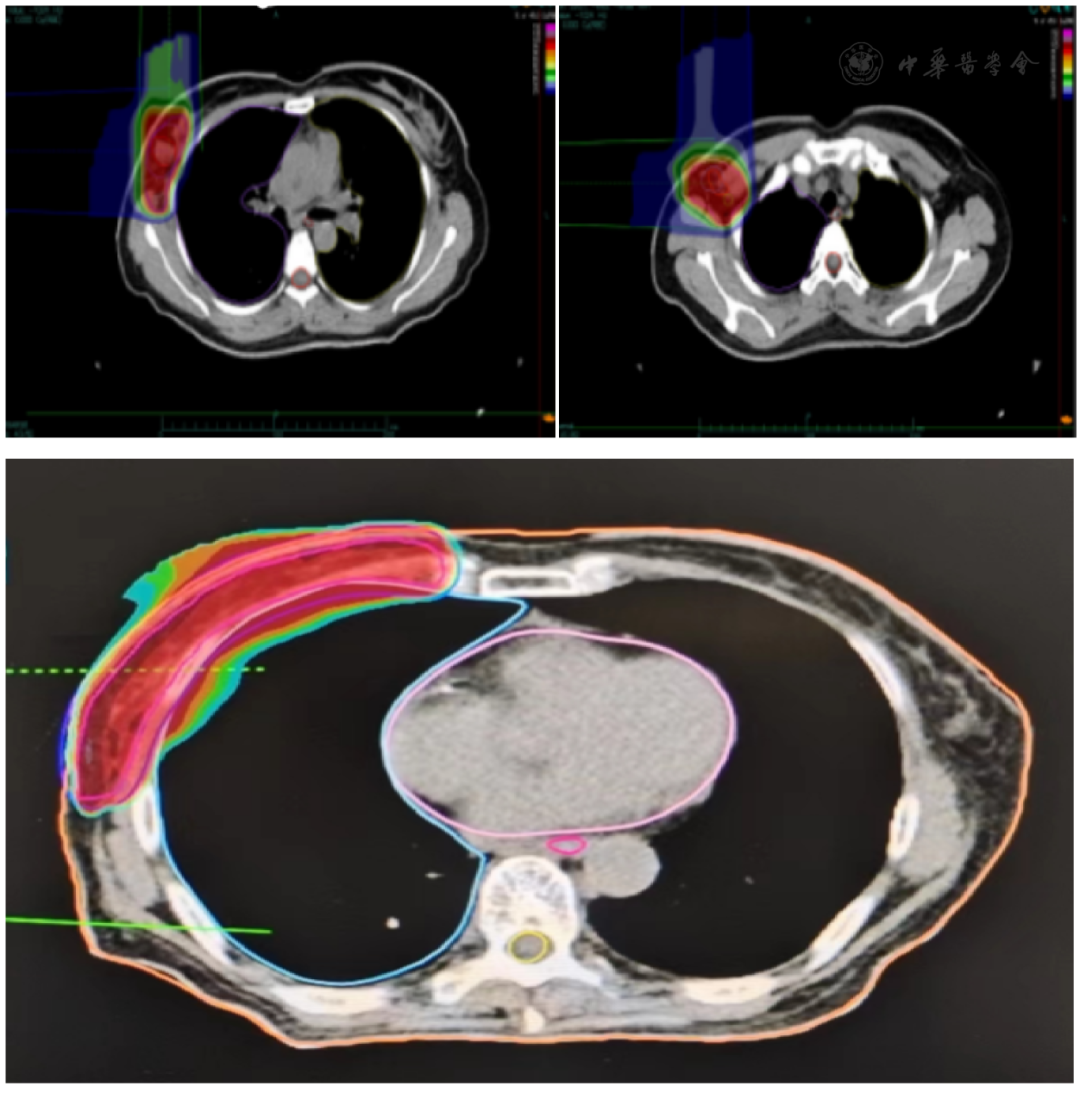
Fig 1 Dose Cloud Map A: Dose cloud map of primary lesion; B: Dose cloud map of axillary lymph node; C: Dose cloud map of chest wall
Fig 2 DVH Diagram
The specific radiotherapy plan was: GTVt was the right breast lesion, GTVn was the right axillary metastatic lymph node; CTVt (GTVt + 0.5 cm), CTVn (GTVn + 0.5 cm), CTV (CTVn + CTVt + right chest wall, right axillary and supraclavicular lymph node drainage areas). The upper border of the right chest wall field was approximately 2 cm above the uppermost edge of the breast tissue and matched the supra/infraclavicular field, the lower border was 2 cm below the breast fold, the posterior border included 1 cm of lung tissue, the anterior border was the anterior breast margin, the medial border was the medial breast tissue margin; the lateral border matched the axillary field. The supra/infraclavicular field's upper border was at the level of the cricothyroid membrane, the lower border matched the chest wall field, the medial border was the medial border of the sternocleidomastoid muscle, the lateral border was the medial border of the humeral head. The axillary field matched the supra/infraclavicular fields and the chest wall field, its lower border was at the second intercostal space, the lateral border included the humeral neck. PTV (CTV + 0.5 cm). PTV [48 Gy (RBE)/12 Fx], PTVn [60 Gy (RBE)/12 Fx], PTVt [72 Gy (RBE)/12 Fx]; 90% of the PTV received 90% of the prescription dose. Dose constraints for organs at risk: Esophagus [Dmax=1.9 Gy (RBE)], Right Lung [D20%=1.5 Gy (RBE)], Spinal Cord [Dmax=0.3 Gy (RBE)]. Regarding comprehensive therapy, the patient refused chemotherapy. According to CSCO Breast Cancer Guidelines, endocrine therapy is feasible for hormone receptor-positive patients who cannot tolerate chemotherapy, refuse chemotherapy, or have poor response to chemotherapy. Therefore, the patient was given endocrine therapy with "Tamoxifen Citrate Tablets 10 mg/dose, twice daily" and ovarian suppression therapy with "Goserelin Acetate Sustained-Release Implant 3.6 mg, subcutaneous injection, once every 4 weeks".
Treatment Outcome, Follow-up, and Prognosis
Upon re-examination after treatment completion, the patient's right breast primary lesion reduced from 2.5 cm×1.7 cm to 2.1 cm×1.2 cm (Fig 3A, B), and the right axillary metastatic lymph node reduced from 1.2 cm×0.6 cm to 0.8 cm×0.5 cm (Fig 3C, D). According to RECIST 1.1 criteria: SD (Stable Disease). According to RTOG criteria, at the end of treatment, the patient had mild skin pigmentation in the right axilla and breast, indicating Grade 1 acute skin reaction. Three weeks after treatment completion, the patient developed patchy moist desquamation in the skin of the right axilla and breast, indicating Grade 2 acute skin reaction. The acute skin reaction subsided and gradually resolved after treatment. Follow-up visits were conducted as scheduled. Nine months after treatment completion, a chest CT re-examination showed complete disappearance of the lesions without distant metastasis (Fig 3E, F). According to RECIST 1.1 criteria: CR (Complete Response).
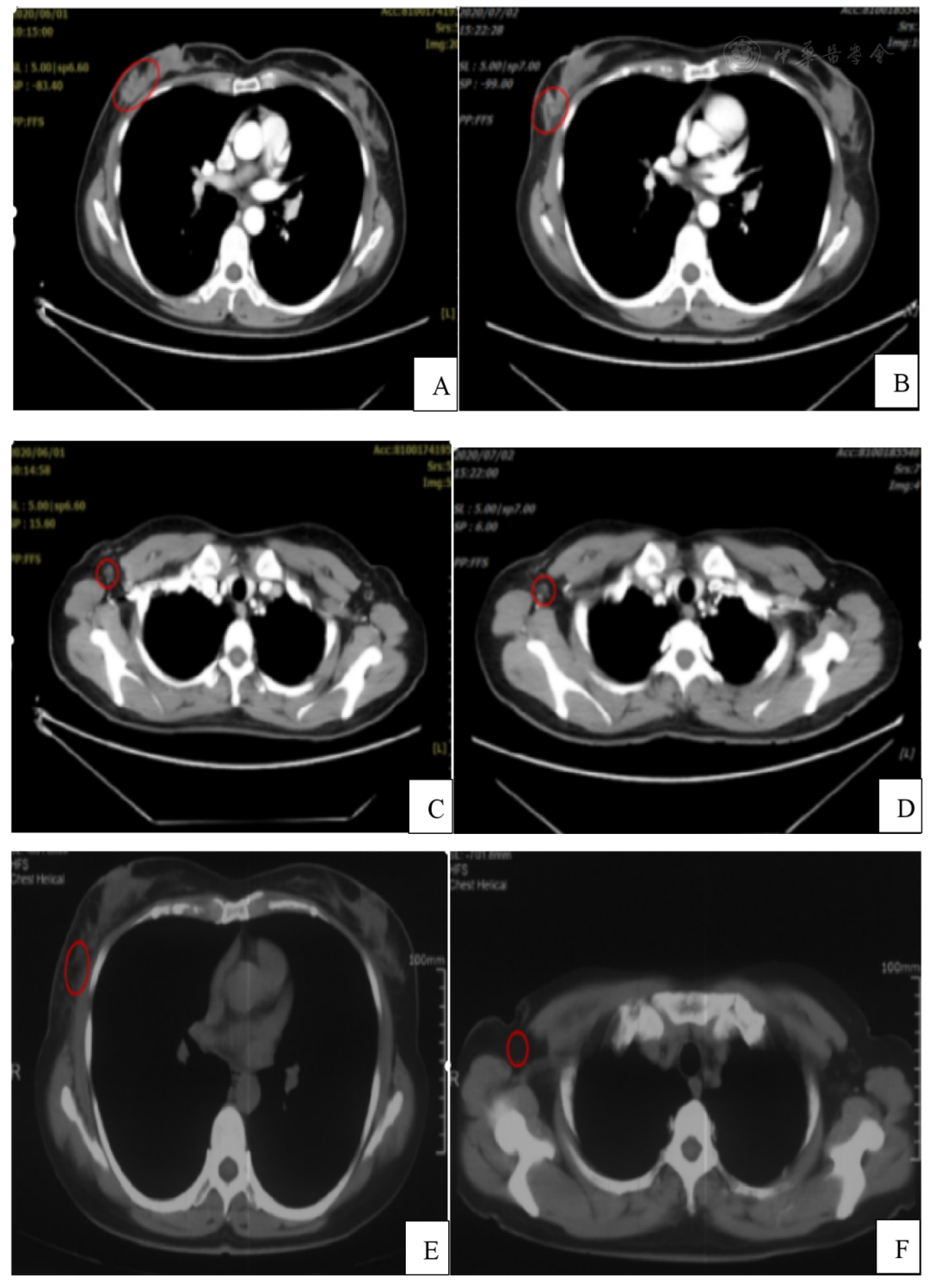
Fig 3 Patient Chest CT
A: Right breast primary lesion before treatment; B: Right breast primary lesion after treatment; C: Right axillary metastatic lymph node before treatment; D: Right axillary metastatic lymph node after treatment; E: Disappearance of right breast mass 9 months after treatment; F: Disappearance of right axillary metastatic lymph node 9 months after treatment
Discussion
Regarding carbon ion therapy for breast cancer, a clinical study on local carbon ion radiotherapy for stage I breast cancer was conducted in Japan from April 2013 to November 2015. Except for one high-grade case, tumors completely disappeared. For stage I breast cancer patients, carbon ion radiotherapy is considered effective and safe through careful patient selection. In 2014, Japan published the world's first case report of carbon ion therapy for early-stage breast cancer. Only Grade 1 skin reaction occurred during treatment, and the dose to the lungs, heart, and contralateral breast was minimal or undetectable, demonstrating the low damage to surrounding normal tissues and organs during carbon ion therapy. It provides another treatment option for breast cancer patients unwilling to undergo surgery and serves as a reference for radical radiotherapy for breast cancer in other institutions worldwide. Of course, directly choosing carbon ion radiotherapy for patients unwilling to undergo surgery requires more case numbers and long-term follow-up for confirmation.
This case involved a Stage IIB breast cancer patient who refused surgery and chemotherapy and directly received carbon ion radiotherapy, concurrently with endocrine therapy. Recent follow-up data show complete disappearance of the right breast mass and axillary lymph nodes without distant metastasis, achieving a recent treatment efficacy of CR. However, the patient experienced Grade 2 acute skin reaction after treatment. The primary reason analyzed is the proximity of the breast lesion and enlarged axillary lymph node to the skin, resulting in a slower dose fall-off. Secondly, in the early stage of our center's operation, only passive beam scanning was available, preventing intensity modulation, leading to higher doses anterior to the target volume along the beam path. Therefore, how to protect breast and axillary skin during carbon ion radiotherapy is another issue requiring exploration.
The chest CT follow-up 9 months post-treatment showed complete disappearance of the lesions, achieving a perfect cosmetic outcome. This represents the most significant difference from surgical treatment. Surgery requires general anesthesia, results in surgical scarring, and may even involve mastectomy, which can be difficult for some women to accept. Within 1~3 months after carbon ion radiotherapy, the tumor gradually shrinks until it becomes impalpable. Post-treatment adverse reactions are relatively mild, and patient compliance and comfort are good.
Non-surgical treatments for breast cancer include radiofrequency ablation, cryoablation, and stereotactic body radiotherapy (SBRT). Radiofrequency ablation has been reported the most. Ito et al. reported 5-year in-breast recurrence-free rates of 97%, 94%, and 87% for 386 patients treated with radiofrequency ablation across 10 centers from 2003 to 2009. Nguyen et al. reviewed 643 radiofrequency ablation cases from 30 studies, with complete ablation rates ranging from 100% to 44%, with a median of 88%. For cryoablation, Lanza et al. reviewed 7 studies from 2003 to 2013, totaling 176 cases, finding complete local tumor control achieved in 73%. Reports on radical SBRT are even fewer. Shibamoto et al. reported the treatment efficacy of 18 patients who refused surgery, received whole breast irradiation plus SBRT boost combined with the radiosensitizer KORTUC, with only one case of local recurrence. Regarding carbon ion therapy for breast cancer, a study from the Japanese NIRS center on Stage I breast cancer reported a prospective phase I trial of 7 Stage I breast cancer patients treated with carbon ions. Enrolled patients were over 60 years old, with an expected survival of 6 months, tumor stage I, single tumor diameter less than 2 cm, IHC expression ER positive, HER2 negative. Patients tolerated the treatment well. Four patients developed acute Grade 1 skin toxicity, with no other toxicities. At 3-month follow-up, 1 patient achieved CR, 5 patients achieved partial response (PR), and 1 patient had stable disease (SD). Six patients received endocrine therapy post-treatment. After 37~48 months of follow-up, no patient had recurrence. In contrast, this patient, 54 months after carbon ion therapy, shows no clinical abnormalities based on current follow-up. Moreover, the dose received by her organs at risk was far below normal limits. She only experienced Grade 2 acute skin reaction, which subsided and resolved after treatment, with no other treatment-related adverse reactions occurring throughout the entire course. Compared to radiofrequency ablation, cryoablation, and SBRT, carbon ion radiotherapy has the advantages of high tumor control and low adverse events.
Carbon ion therapy has not yet been widely applied to breast cancer treatment. Although related research is limited, CIRT possesses distinct physical and biological characteristics that may benefit a large number of breast cancer patients in the future. Carbon ion beams deposit a large amount of energy upon entering the human body, forming a Bragg peak that precisely conforms the high-dose region to the tumor target. This physical characteristic provides not only higher precision in dose distribution compared to photon radiotherapy but also significantly better protection of normal tissues. Carbon ions also have the feature of high linear energy transfer (LET), higher relative biological effectiveness (RBE), and a lower oxygen enhancement ratio. These advantages can further enhance tumor cell kill and treatment safety.
With economic development and increasing demands for disease treatment, more and more breast cancer patients not only require improved survival but also demand minimal treatment adverse reactions. Therefore, radical carbon ion therapy for breast cancer is a new research topic. Currently, due to the cost of treatment and limited number of facilities, carbon ion radiotherapy for breast cancer remains a limited treatment modality. Based on the short-term efficacy observed in this breast cancer patient treated at our institution, clinical research on carbon ion radiotherapy for breast cancer has promising exploration prospects. For some breast cancer patients who refuse surgical treatment, direct carbon ion radiotherapy shows significant short-term efficacy with tolerable toxicity. However, whether the local control rate can reach the level of surgical treatment requires longer follow-up time for confirmation.
Carbon Ion Radiotherapy (CIRT) is an advanced radiotherapy technique that uses high-energy carbon ion particle beams to damage the DNA of tumor cells, thereby inhibiting their growth and proliferation. Unlike conventional radiotherapy, which primarily uses photon radiation (such as X-rays and gamma rays), CIRT utilizes heavy ions, specifically carbon ions, which possess unique physical and biological properties that make it more effective in treating certain types of tumors.
Authors: Zhang Yihe, Zhang Yanshan, Pan Xin, Wang Xin, Yang Yuling, Ma Tong, He Nana, Ma Xiaoyun, Li Wanguo
2025,07(01):E0137-E0137. DOI:10.3760/cma.j.cmcr20241024-02240
Source: Zhang YH, Zhang YS, Pan X, et al. A case of breast cancer patient treated with carbon ion radiotherapy. Chinese Clinical Case Results Database, 2025, 07(01): E0137-E0137. DOI: 10.3760/cma.j.cmcr20241024-02240
Editor: Ricker
Should any copyright issues be involved, please contact the authors, and we will address them promptly. Thank you!

