
Dosimetric Comparison of Carbon Ion Radiotherapy with Photon Radiotherapy for Thoracic Vertebral Met
Dosimetric Comparison of Carbon Ion Radiotherapy with Photon Radiotherapy for Thoracic Vertebral Metastatic Carcinoma
JIN Xue-ling, MA Xiao-yun, ZHANG Meng-ling, ZHANG Yan-shan, SHI Zi-ke, QIN Tian-yan
(Gansu Wuwei Cancer Hospital, Wuwei, Gansu 733000)
Abstract:
[Objective] To compare the dosimetric advantages of carbon ion radiotherapy (CIRT) with photon-based three-dimensional conformal radiotherapy (3DCRT), intensity-modulated radiotherapy (IMRT), and volumetric modulated arc therapy (VMAT) plans in vertebral metastases.
[Methods] Four radiotherapy plans (CIRT, 3DCRT, IMRT, and VMAT) were designed for 10 patients with thoracic vertebral metastases. Target delineation followed the recommendations of the International Commission on Radiation Units and Measurements (ICRU) Reports No. 50, 62, and 83. Photon treatment plans were generated using the Eclipse planning system, while carbon ion plans were created with the ciPlan system (all 2D conformal carbon ion plans). The optimization constraints were largely identical, requiring 95% prescription dose coverage of the planning target volume (PTV). The conformity index (CI) and homogeneity index (HI) were used to evaluate target dose distribution and conformity. The gradient index (GI) and the ratio of the 5 Gy isodose volume to PTV volume (V5/VPTV) assessed the dose falloff outside the target. Parameters such as mean dose (Dmean), maximum dose (Dmax), and 5 Gy isodose volume (V5) evaluated organ-at-risk (OAR) doses.
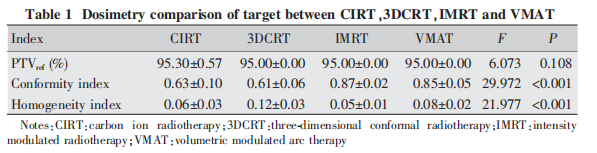
[Results] All four plans (CIRT, 3DCRT, IMRT, and VMAT) met clinical dosimetric requirements. The prescription dose coverage rates were: CIRT 95.30% ± 0.57%, and 95% for 3DCRT, IMRT, and VMAT. Among the four plans, 3DCRT showed statistically significant differences in HI compared to the other three groups (P < 0.001). For CI, significant differences were observed between the 3DCRT/CIRT groups and the VMAT/IMRT groups (P < 0.001). CIRT demonstrated significantly lower GI and V5/VPTV than any photon-based plan (P < 0.001). Doses to OARs such as the liver, small intestine, heart, and stomach were relatively low, but without statistical significance. Spinal cord doses varied with the maximum target dose, also without statistical significance. CIRT not only reduced the mean lung dose but also significantly decreased the low-dose lung irradiation volume.
[Conclusion] Compared with 3DCRT, IMRT, and VMAT photon plans, CIRT effectively reduces radiation exposure to both lungs while maintaining target prescription dose coverage and dose homogeneity in thoracic vertebral metastases.
Keywords: Thoracic vertebral metastases; Carbon ion radiotherapy; Photon radiotherapy; Dosimetry
Chinese Library Classification (CLC): R730.55
Document Code: B
Article ID: 1671-170X(2022)05-0424-04
DOI: 10.11735/j.issn.1671-170X.2022.05.B014
Vertebral metastases are the third most common type of metastatic cancer after lung and liver metastases. These tumors can destroy normal bone tissue, leading to symptoms such as pain, hypercalcemia, pathological fractures, and nerve compression. Most patients with vertebral metastases receive radiotherapy primarily for palliative purposes. Radiotherapy not only alleviates pain, prevents pathological fractures, and halts local disease progression, but may also facilitate neurological function recovery, making it the preferred treatment for vertebral metastases [1-10].
Carbon ion radiotherapy (CIRT) offers significant physical advantages by providing more effective protection to normal tissues. After entering the body, the radiation deposits a high concentration of energy within an extremely short time window in the tumor region, forming a narrow and steep Bragg peak, followed by rapid energy decay. The depth of the Bragg peak is determined by the energy of the radiation. Additionally, carbon ions are high linear energy transfer (LET) particles, and their high LET characteristics enable direct double-strand DNA breaks, thereby enhancing therapeutic efficacy—particularly against tumor cells that exhibit resistance to photon-based treatments.
Carbon ions also have a limited penetration range, an amplification effect of at least 5–6 times, and the ability to kill tumor cells independent of the cell cycle or oxygen environment. Clinically, single or multiple fractionation regimens can be flexibly selected based on the condition of surrounding normal tissues. Moreover, carbon ions exhibit immunoenhancing effects, abscopal effects, and bystander effects, which contribute to their increasing global acceptance and recommendation [11-12].
1 Materials and Methods
1.1 Patients and Image Acquisition
From August 2020 to April 2021, 10 patients with thoracic vertebral metastases at the Heavy Ion Center of Wuwei Cancer Hospital, Gansu Province, received one of the following radiotherapy modalities: three-dimensional conformal radiotherapy (3DCRT), intensity-modulated radiotherapy (IMRT), volumetric modulated arc therapy (VMAT), or carbon ion radiotherapy (CIRT). Patients underwent CT simulation in either the supine or prone position, with a 4-hour fasting period before positioning and 3-mm slice thickness scanning. CT images were transferred to the treatment planning system and fused with MRI scans for target delineation. Target delineation followed the guidelines of the International Commission on Radiation Units and Measurements (ICRU) Reports No. 50, 62, and 83.
1.2 Target Definitions
The gross tumor volume (GTV) was primarily defined based on CT, contrast-enhanced MRI, and PET-CT imaging. The clinical target volume (CTV) was generated by expanding the GTV by 5 mm to cover subclinical lesions, with a minimum expansion of 1 mm at critical organs. To account for setup errors and dose distribution uncertainties, the planning target volume (PTV) was created by adding a 3–6 mm margin around the CTV.
1.3 Treatment Planning
CIRT plans were designed using the ciPlan heavy ion treatment planning system, while 3DCRT, IMRT, and VMAT plans were generated using the Eclipse 15.6 treatment planning system. In this study, the prescribed dose for CIRT was 30 Gy in 10 fractions (30 Gy/10 F), the same as for 3DCRT, IMRT, and VMAT. The 95% isodose line was required to cover the PTV. All treatment plans were developed collaboratively by at least two physicians, one dosimetrist, and one senior medical physicist.
1.4 Study Endpoints
The primary endpoints included target dose coverage, conformity index (CI), homogeneity index (HI), gradient index (GI), and low-dose contribution metrics.
The CI, which quantifies PTV conformity, was calculated using the standard formula (Equation 1), where PTVrefrepresents the target volume enclosed by the prescription isodose line, VPTVis the total target volume, and Vrefis the volume encompassed by the prescription isodose line. A CI value closer to 1 indicates better conformity.

The homogeneity index (HI) expression is as follows (Equation 2), where D2 is the dose received by 2% of the target volume, D98 is the dose received by 98% of the target volume, and D50 is the dose received by 50% of the target volume. The closer the HI value is to 0, the better the dose homogeneity.
The gradient index (GI) expression is as follows (Equation 3), which evaluates the dose falloff outside the target volume, where PIV1/2 is the volume enclosed by the 50% prescription dose isodose line, and PIV is the volume enclosed by the prescription dose isodose line.

The low-dose contribution is calculated using Equation (4), where V5 is the volume enclosed by the 5 Gy isodose line and VPTV is the planning target volume.

For the PTV and organs at risk (OARs), the dose distribution and dose-volume histogram (DVH) were evaluated. Each organ at risk and each treatment plan were assessed using parameters including the mean dose (Dmean) and the volume receiving a specific fixed dose (e.g., V5 of the lungs refers to the lung volume receiving 5 Gy).
1.5 Statistical Analysis
Statistical analysis was performed using SPSS 22.0 software. Measurement data are expressed as mean ± standard deviation, and analyzed by t-test or analysis of variance (ANOVA). If the conditions for t-test or ANOVA were not met, non-parametric tests were used. The significance level was set at α = 0.05.
2 Results
2.1 Target Dose Coverage
The target coverage rate was 95.30% ± 0.57% for CIRT plans, and 95% for 3DCRT, IMRT, and VMAT plans. There was no statistically significant difference in CI between CIRT plans and 3DCRT plans; however, the CI of IMRT and VMAT plans was superior to the other two groups (P < 0.001). No statistically significant difference in HI was observed among the CIRT, IMRT, and VMAT groups, but all showed significant differences compared with 3DCRT (P < 0.001) (Table 1).
2.2 Dose Gradient Outside the Target
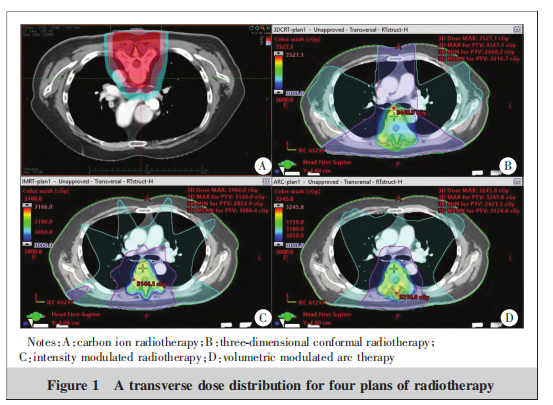
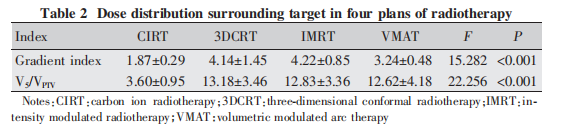
In the dose distribution screenshot (Figure 1), the outermost blue curve represents the 5 Gy isodose line, the middle pink curve represents half of the prescription dose (i.e., the 15 Gy isodose line), and the red area in Figure a as well as the solid dose display areas in Figures b, c, and d all represent the region covered by the prescription dose of 30 Gy. It can be observed that the low-dose volume distributions of the three photon plans are similar, while the low-dose volume of normal tissues outside the target in the heavy ion plan is significantly smaller than that in the photon plans. As shown in the data for the GI and low-dose contribution of the 10 plans (Table 2), the GI and V5/VPTV values of the heavy ion plan are significantly lower than those of the photon plans (P < 0.001).
2.3 Organ-at-Risk Doses
In the four treatment plans, the radiation doses to organs at risk (OARs) including the kidneys, stomach, and small intestine were low and showed no statistically significant differences. No significant difference was observed in the maximum spinal cord dose between the CIRT and IMRT plans; however, the CIRT plan delivered a significantly lower spinal cord dose compared to the 3DCRT and VMAT plans (P < 0.001). Although the difference in spinal cord dose was statistically significant, it was not clinically meaningful, and the trend of spinal cord dose correlated with the maximum target dose (Table 3).
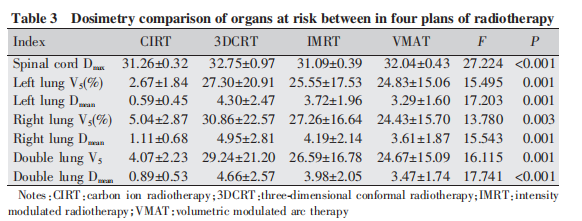
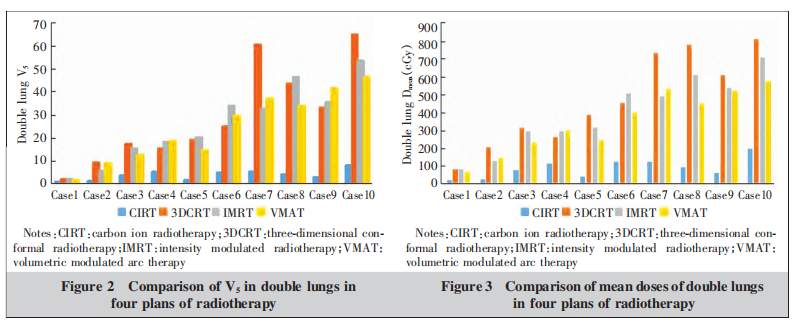
The left and right lung V5 and Dmean values in the CIRT plans were significantly better than those in the 3DCRT, IMRT, and VMAT plans (P < 0.001 for all). Histogram analysis of lung Dmean and V5 (Figures 2-3) clearly shows that among the three photon plans, both the low-dose volume and mean dose of the lungs exhibited a positive correlation with the proportion of lung slices occupied by the target. However, the carbon ion plan significantly reduced the low-dose volume and mean dose of both lungs, with particularly notable differences in cases where the target occupied more lung slices. In the CIRT plans, both the mean lung dose and low-dose volume were substantially lower than those in the 3DCRT, IMRT, and VMAT photon plans, demonstrating a clear trend where the higher the lung dose in photon plans, the more pronounced the differences became.
3 Discussion
Based on the comparative results of the target volumes, the conformity index (CI) of IMRT and VMAT plans was significantly better than that of CIRT and 3DCRT. Although there were no statistically significant differences in the homogeneity index (HI) among the CIRT, IMRT, and VMAT groups, all three showed clear advantages over 3DCRT. Therefore, the CIRT plan demonstrates dosimetric superiority for target volume coverage compared to the 3DCRT plan.
The gradient index (GI) and V5/VPTV of the carbon ion plan were both significantly lower than those of the three photon plans, and its homogeneity index outperformed that of 3DCRT, which is also a conformal plan. These findings highlight the unique physical advantages of carbon ion beams. However, the CI of the carbon ion plan was inferior to that of IMRT and VMAT, primarily because we employed uniform scanning without incorporating comprehensive target conformity optimization in the planning system. This indicates substantial potential for further improvement in carbon ion planning.
Beyond physical advantages, carbon ion therapy also offers biological benefits. It can directly induce DNA double-strand breaks, is unaffected by the radioresistance of hypoxic cells, and is not influenced by dose fractionation effects related to cellular repair mechanisms—making it more therapeutically favorable for patients.
A key dosimetric advantage of carbon ions is the reduction in irradiated volume, with the volume of normal tissues, particularly low-dose regions, being significantly lower than that of photon plans. In the thoracic vertebral metastases cases studied, the lung’s low-dose volume (V5) and mean dose (Dmean) directly determine the probability of radiation pneumonitis [13].
For photon plans, if a large number of vertebral bodies are irradiated and they all lie within the lung levels, the low-dose volume may become very large. In contrast, the carbon ion plan contributes minimally to the lung’s low-dose exposure, showing almost no correlation with the proportion of lung levels occupied by the target. In one selected case, the photon plan resulted in a maximum bilateral lung V5 of 65.03%, whereas the carbon ion plan for the same case achieved a bilateral lung V5 of only 8.25%.
These findings demonstrate that for patients with vertebral metastases—especially those involving multiple thoracic vertebral segments with longer target volumes—carbon ion therapy can substantially reduce the risk of radiation pneumonitis. Thanks to its ability to minimize irradiated volumes, carbon ion therapy also provides significant advantages in protecting surrounding organs. Future research should further optimize carbon ion radiotherapy techniques to benefit more cancer patients.
References:
[1] Zaikova O, Fosså SD, Kongsgaard U, et al. Pain after palliative radiotherapy for spine metastases [J]. Clin Oncol (R Coll Radiol), 2010, 22(10): 828-836.
[2] 许珍, 于甬华. 脊柱转移瘤放疗研究进展[J]. 中华肿瘤防治杂志, 2020, 23(1): 80-84.
Xu Z, Yu YH. Advances in radiotherapy of spinal metastases[J]. Chinese Journal of Cancer Prevention and Treatment, 2020, 23(1): 80-84.
[3] 崔云鹏, 施学东. 脊柱转移瘤治疗进展[J]. 肿瘤防治研究, 2018, 45(5): 337-342.
Cui YP, Shi XD. Progress of treatment on metastatic spinal tumors [J]. Cancer Research on Prevention and Treatment, 2018, 45(5): 337-342.
[4] 王华强, 滕勇. 脊柱转移瘤治疗进展[J]. 国际骨科学杂志, 2015, 36(1): 22-25.
Wang HQ, Teng Y. Progress in the treatment of vertebra metastases carcinoma[J]. International Journal of Orthopaedics, 2015, 36(1): 22-25.
[5] 刘慧云, 刘东胜. 不同分割方式放疗治疗骨转移肿瘤的临床疗效[J]. 肿瘤基础与临床, 2020, 33(2): 107-109.
Liu HY, Liu DS. Clinical efficacy of radiotherapy with different segmentation methods in the treatment of bone metastases[J]. Journal of Basic and Clinical Oncology, 2020, 33(2): 107-109.
[6] Sprave Τ, Verma V, Förster R, et al. Quality of life following stereotactic body radiotherapy versus three-dimensional conformal radiotherapy for vertebral metastases: secondary analysis of an exploratory phase Ⅱ randomized trial[J]. Anticancer Res, 2018, 38(8): 4961-4968.
[7] Baba S, Matsumoto Y, Kawaguchi K, et al. Post-carbon-ion radiotherapy vertebral pathological fractures in upper cervical primary malignant spinal tumors treated by occipitocervical fusion[J]. Arch Orthop Trauma Surg, 2019, 139(11): 1525-1531.
[8] 陈仁金, 杨波, 孙小杨, 等. 脊柱转移瘤调强放射治疗发泡剂泡沫垫和热塑体膜固定技术临床应用比较[J]. 中华肿瘤防治杂志, 2020, 27(16): 1335-1339.
Chen RJ, Yang B, Sun XY, et al. Analysis in intensity modulated radiotherapy for spinal metastases using two immobilization devices[J]. Chinese Journal of Cancer Prevention and Treatment, 2020, 27(16): 1335-1339.
[9] 徐敏仙, 欧晋, 周弘达. 胸椎转移瘤 3D-CRT 与 IMRT 治疗技术比较[J]. 湘南学院学报(医学版), 2021, 23(1): 38-41.
Xu MX, Ou J, Zhou HD. Comparison of 3D-CRT and IMRT technique on thoracic vertebra metastasis[J]. Journal of Xiangnan University (Medical Sciences), 2021, 23(1): 38-41.
[10] 董海权, 李永春, 肖锋, 等. 自动计划与手动计划在椎体骨转移癌调强放射治疗中的剂量学比较[J]. 医疗装备, 2020, 33(15): 3-5.
Dong HQ, Li YC, Xiao F, et al. Dosimetric comparison of automatic planning and manual planning in intensity modulated radiotherapy for vertebra metastases[J]. Medical Equipment, 2020, 33(15): 3-5.
[11] 张雁山, 王慧娟, 叶延程, 等. 碳离子束放射治疗肿瘤的临床进展[J]. 医学综述, 2017, 23(20): 4033-4044.
Zhang YS, Wang HJ, Ye YC, et al. Clinical progress of carbon ion beam radiotherapy for tumor[J]. Medical Recapitulate, 2017, 23(20): 4033-4044.
[12] 张雁山, 叶延程, 张红. 碳离子束放射治疗肿瘤的临床进展[J]. 科技促进发展, 2020, 16(1): 18-33.
Zhang YS, Ye YC, Zhang H. Clinical progress of carbon ion radiotherapy for tumors[J]. Science and Technology for Development, 2020, 16(1): 18-33.
[13] 张彦秋, 韩阿蒙, 李金旺, 等. 容积旋转调强放射治疗肺癌患者放射性肺炎发生的相关因素分析[J]. 中国医学物理学杂志, 2018, 35(7): 771-775.
Zhang YQ, Han AM, Li JW, et al. Analysis of factors predicting radiation pneumonitis in volumetric modulated arc therapy of lung cancer[J]. Chinese Journal of Medical Physics, 2018, 35(7): 771-775.
Preliminary Review: Zhang Jie
Final Review: Ma Shuqian

